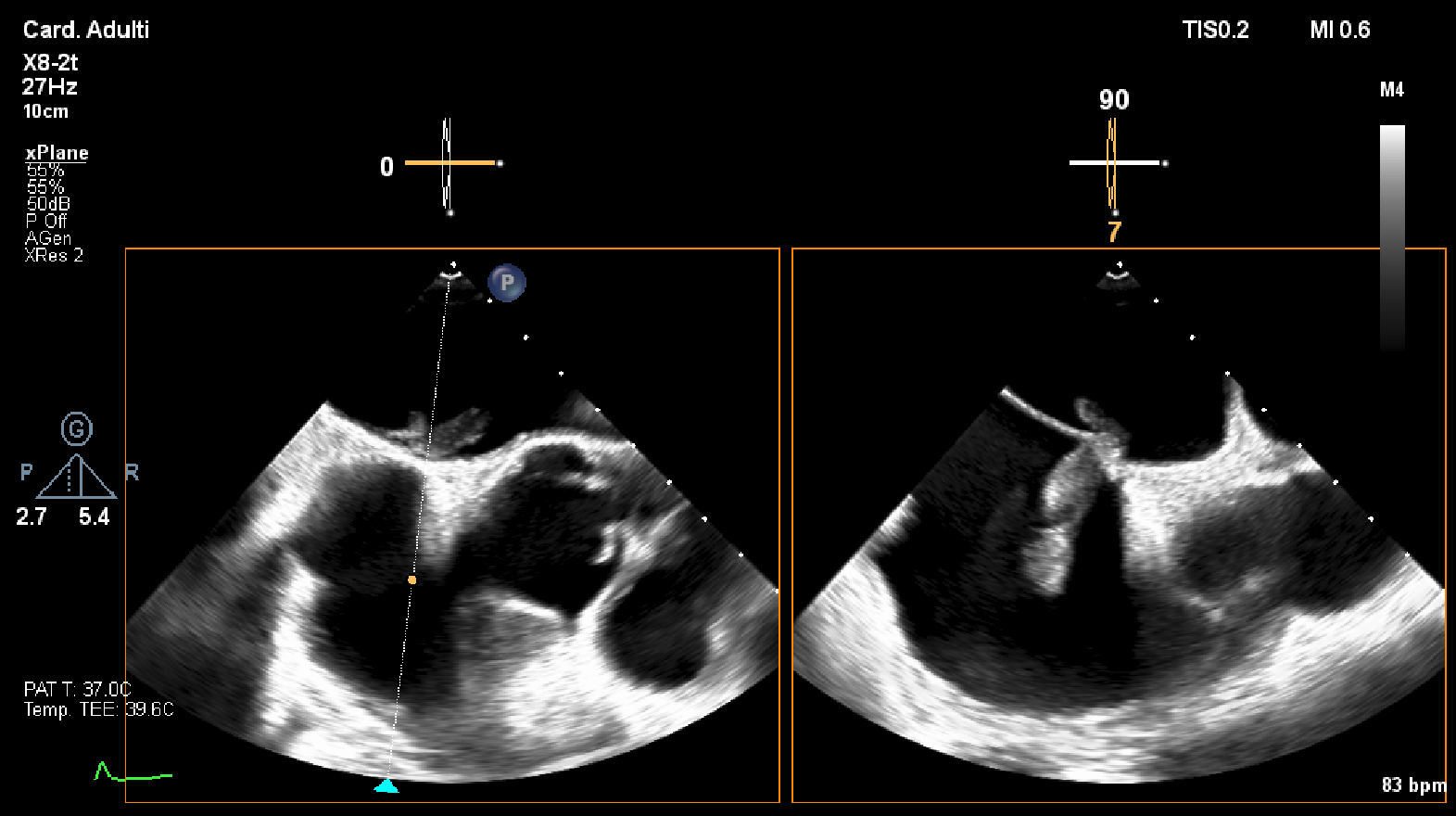
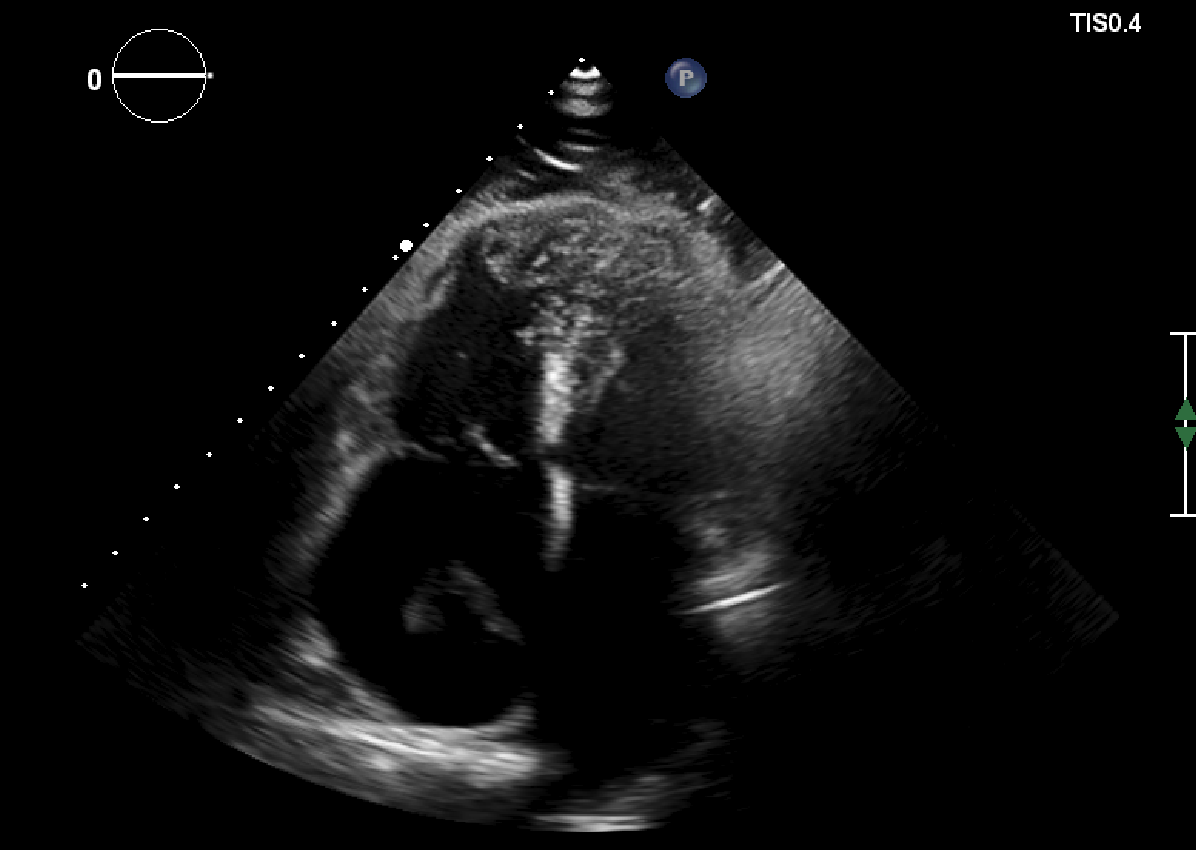
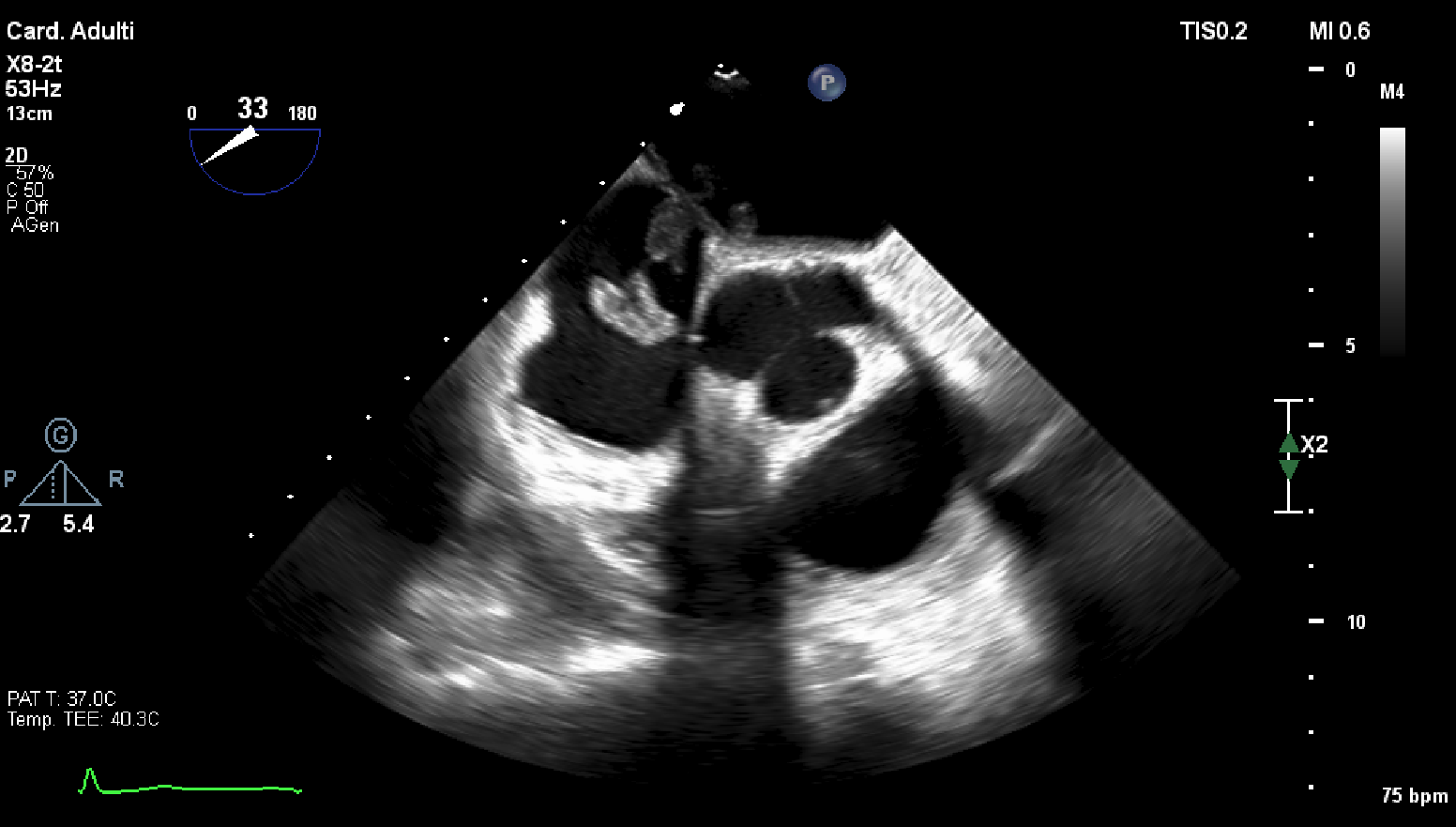
Background: Massive pulmonary embolism complicated by an intracardiac thrombus straddling a patent foramen ovale (PFO) is a rare but life-threatening condition, associated with high risk of systemic embolization and mortality. Case presentation: We report the case of a 68-year-old woman with a history of idiopathic left lower limb deep vein thrombosis, who presented with progressive exertional dyspnea, left leg pain and edema, followed by a witnessed syncope preceded by chest discomfort. Computed tomography pulmonary angiography revealed bilateral massive pulmonary embolism with extensive thrombotic involvement of lobar, segmental and subsegmental branches. Transthoracic echocardiography showed right ventricular dilatation and dysfunction with signs of pulmonary hypertension consistent with an intermediate–high risk pulmonary embolism. Transesophageal echocardiography identified a large, mobile, polylobulated thrombus straddling the interatrial septum through a patent foramen ovale, protruding into both atria. The patient remained hemodynamically stable and was managed conservatively with anticoagulation with unfractionated heparin, followed by low-molecular-weight heparin, and subsequently transitioned to vitamin K antagonist therapy. Serial echocardiographic follow-up demonstrated complete resolution of the intracardiac thrombus and normalization of right ventricular function. A diagnostic workup revealed positivity for Factor V Leiden with no evidence of underlying malignancy. Conclusions: This case highlights the importance of early echocardiographic assessment in acute pulmonary embolism to detect rare but high-risk complications such as thrombus-in-transit through a PFO. In selected hemodynamically stable patients, intensive anticoagulation with close imaging follow-up may represent an effective and safe therapeutic strategy.