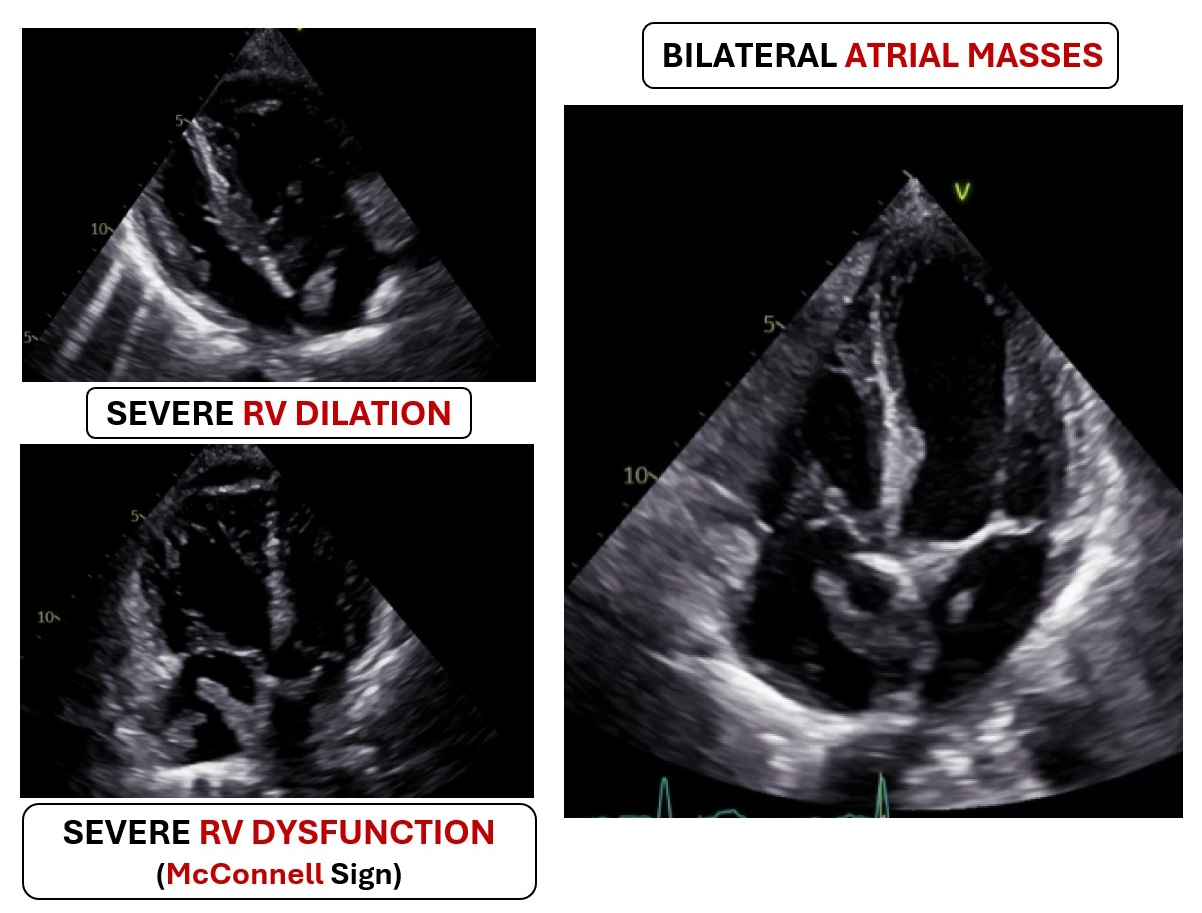
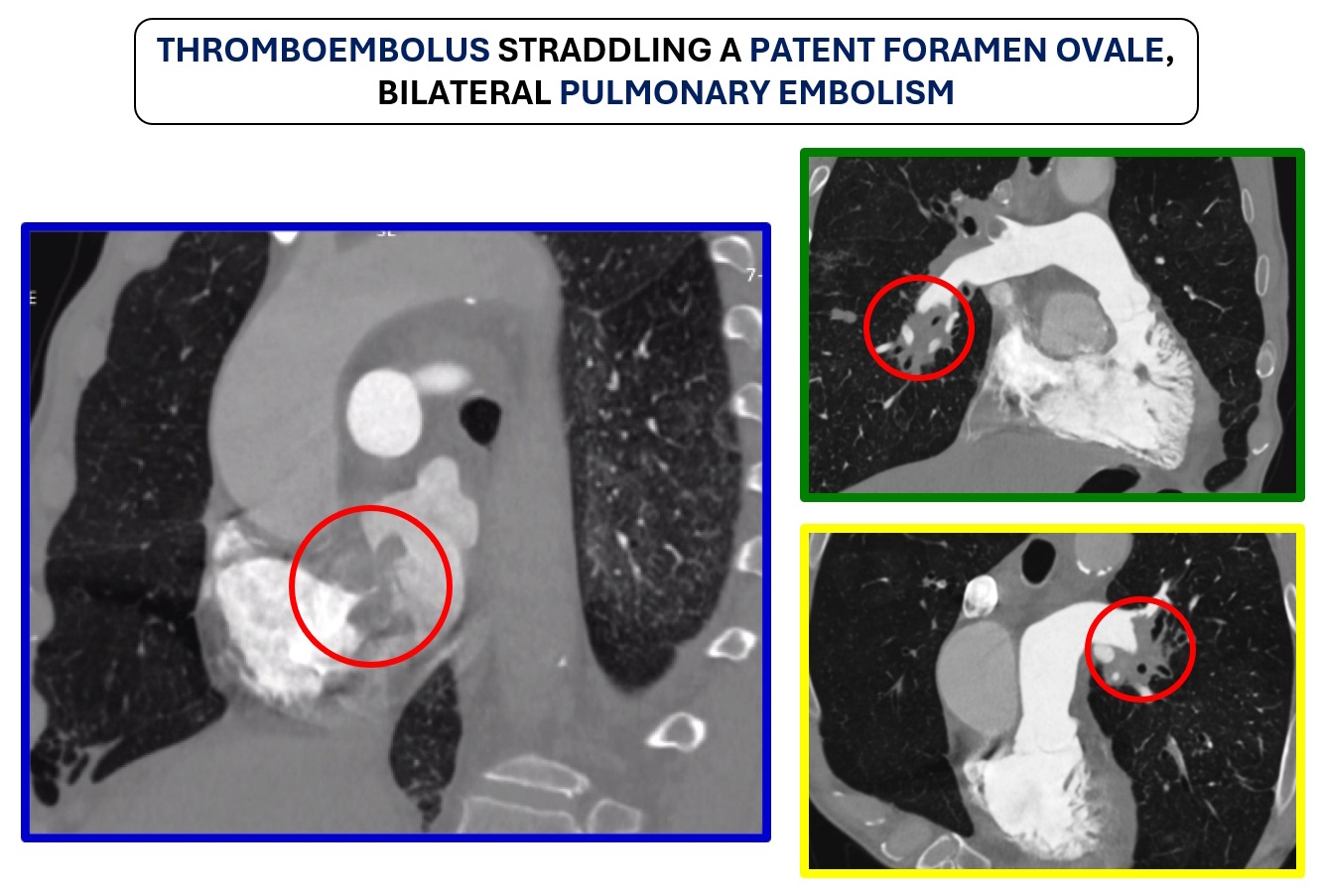
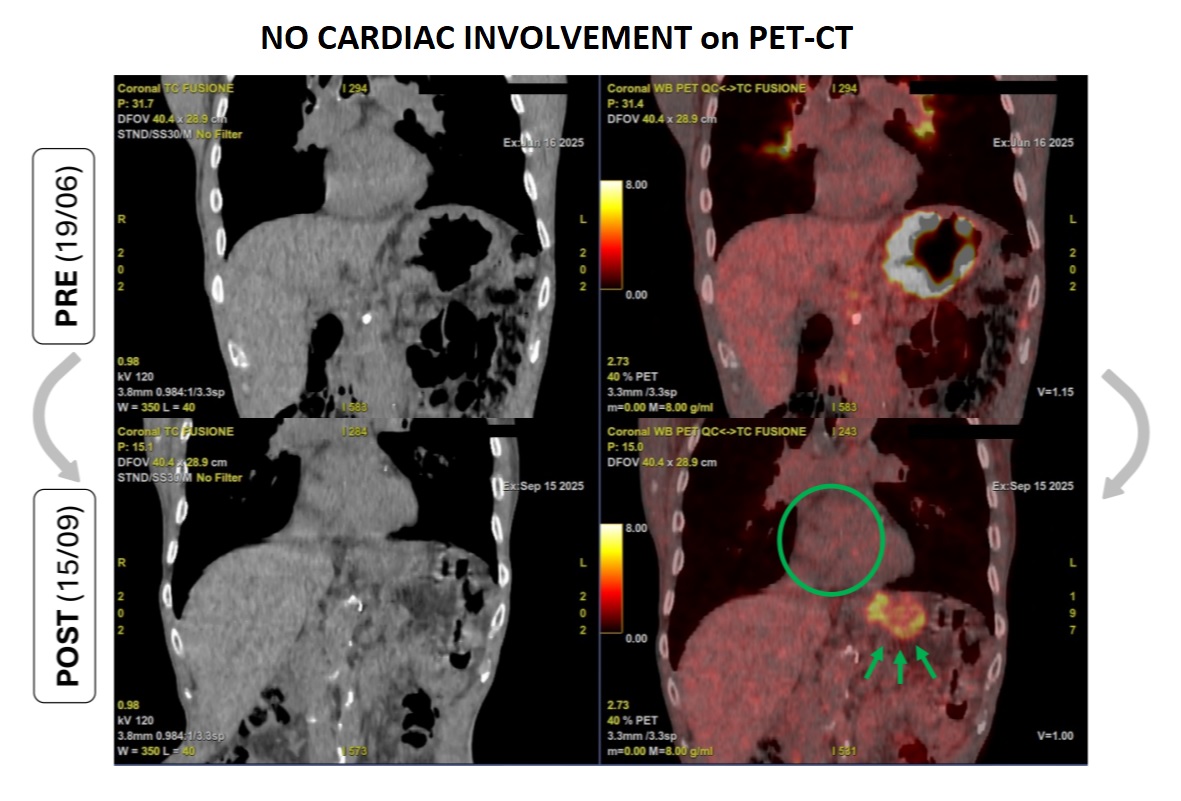
A 76-year-old man with no previous cardiovascular disease was diagnosed with stage IV-B diffuse large B-cell gastric lymphoma and started on chemotherapy. Baseline echocardiography showed preserved left ventricular systolic function, moderate aortic stenosis and intermediate probability of pulmonary hypertension. During treatment, the patient developed progressive clinical deterioration with persistent hypotension, cough, bilateral ankle edema, anorexia and weight loss. Initial laboratory tests revealed neutrophilic leukocytosis with normal cardiac biomarkers, and symptoms were initially attributed to infection and malnutrition. Due to persistent hypotension, a cardiology evaluation was performed and revealed a previously undocumented atrial mass on transthoracic echocardiography. Shortly thereafter, the patient experienced acute worsening with near-syncope and hypoxemic respiratory alkalosis. Electrocardiogram showed T-wave inversion in right precordial leads, while cardiac biomarkers were markedly elevated. Urgent echocardiography demonstrated severe right ventricular dilation and dysfunction with McConnell’s sign, elevated pulmonary artery systolic pressure, and large bilateral atrial masses in contact with the interatrial septum. Computed tomography angiography confirmed bilateral pulmonary embolism and identified a large intracardiac mass extending into both atria, consistent with a thrombus straddling a patent foramen ovale. After multidisciplinary discussion, unfractionated heparin infusion was initiated despite the high bleeding risk related to gastric lymphoma. The patient showed rapid hemodynamic stabilization, progressive recovery of right ventricular function, reduction of pulmonary pressures, and regression of atrial masses. Positron emission tomography excluded cardiac lymphoma involvement. The patient was discharged on oral anticoagulation in stable clinical conditions. In conclusion, pulmonary embolism should be promptly considered in oncological patients with unexplained clinical deterioration; intracardiac masses may mimic malignancy but can be thrombotic; multimodality imaging and individualized multidisciplinary decision-making are crucial in complex cardio-oncology cases.