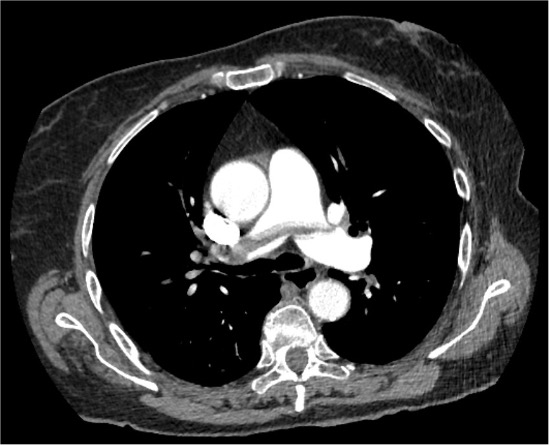
A 75-year-old obese woman with hypertension, type II diabetes, stage IIIa chronic kidney disease and anaemia was admitted after an accidental fall. Hip X-ray showed a right femur fracture, and she underwent uncomplicated hip arthroplasty on day 2. On admission platelet count was 264 x10.9/L and haemoglobin 11.7 g/dL. Thrombotic prophylaxis with low molecular weight heparin (LMWH) 4000 IU/die was started on day 1. On day 10, she developed severe thrombocytopenia (platelets 19 x10.9/L; 12 x10.9/L in citrate) and LMWH was replaced with Fondaparinux; one platelet pool was administered. The following day, she developed acute dyspnoea with hypoxia and hypocapnia. EKG showed right bundle branch block, S1Q3T3 pattern and signs of right ventricular (RV) overload. A contrast-enhanced computed tomography revealed extensive bilateral pulmonary embolism and small subpleural infarcts. She was transferred to the Cardiac Intensive Care Unit. Blood pressure was 115/65 mmHg; heart rate 100 bpm; SpO2 94% on facial mask 10 L/min; respiratory rate 25-30/min; haemoglobin 9.3 g/dL; D-dimer >20 mg/L; troponin T 160 ng/L; NTproBNP 2098 pg/mL. Echocardiography showed RV dilatation and dysfunction, with a TAPSE/sPAP ratio of 0.2. She was classified as intermediate-high risk pulmonary embolism, but thrombolysis was contraindicated due to recent surgery. Suspected heparin-induced thrombocytopenia (HIT) also controindicated unfractionated heparin. The 4Ts score was 5-6 and antibodies against multimolecular complexes of platelet factor 4 (PF4) and heparin complexes were requested. Danaparoid was started after angiologic consultation. Doppler ultrasound revealed bilateral proximal deep vein thrombosis and superficial thrombosis of the right saphenous vein. PF4-heparin antibodies later confirmed HIT. Despite therapy, respiratory and echocardiographic improvement was limited, with persistent oxygen requirement and thrombocytopenia. We consulted the hub centre for catheter-based thrombectomy. After transfusion of two units of red blood cells, the patient underwent successful percutaneous thrombectomy on day 21 with improvement in pulmonary flow. Platelet count gradually improved, allowing the introduction of oral anticoagulant on day 25. At discharge on day 30, echocardiography showed normal dimensions and function of the right ventricle (TAPSE/sPAP was 0.7), EKG abnormalities had resolved, platelet count was 307 x10.9/L, and haemoglobin 11.6 g/dL. Biomarkers markedly improved.