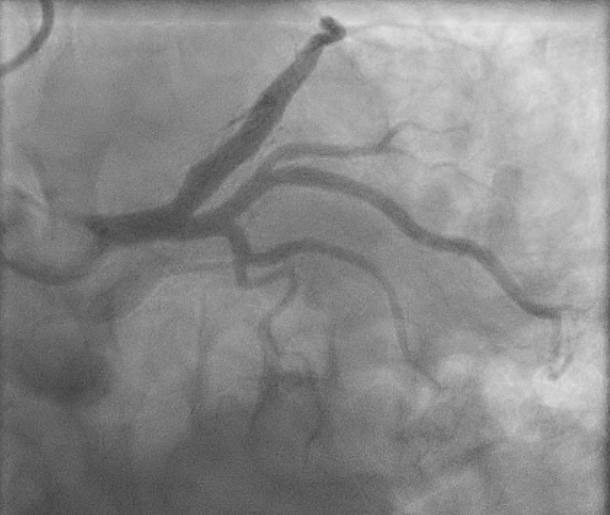
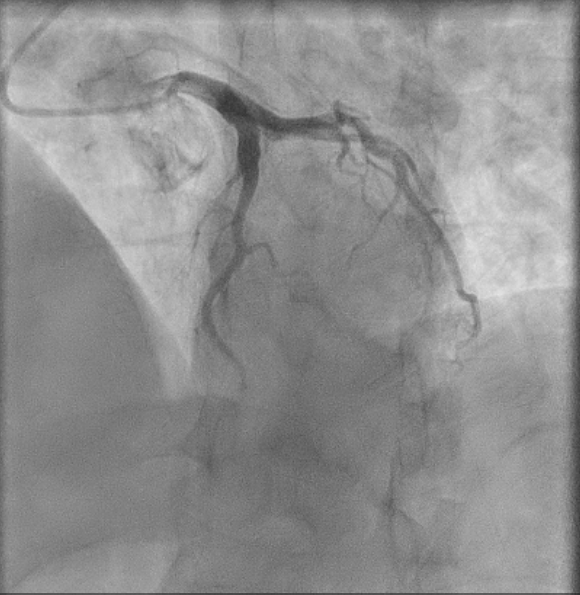
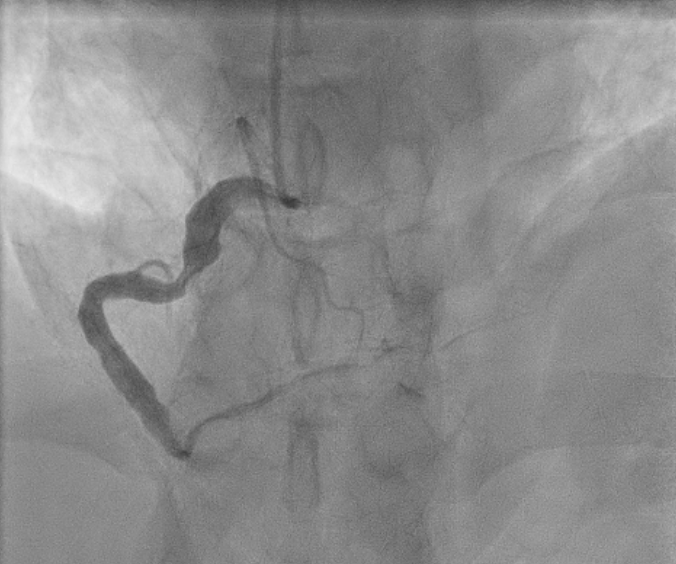
Background: Coronary artery ectasia (CAE) represents an uncommon angiographic finding, defined as a coronary dilatation exceeding 1.5 times the diameter of an adjacent normal segment. CAE may predispose to slow coronary flow, thrombosis, and recurrent ischemic events. Optimal management remains controversial due to the absence of randomized controlled trials and standardized antithrombotic strategies. Case Presentation: A 45-year-old man with hypercholesterolemia, family history of ischemic heart disease presented recurrent episodes of myocardial infarction despite tailored antithrombotic regimens. The first inferior ST-elevation myocardial infarction (STEMI) occurred in 2022 revealing a tortuous, diffusely ectatic right coronary artery (RCA) with slow flow and distal thrombotic occlusion in the absence of atherosclerotic plaque. Thrombophilia testing was negative. The patient was discharged on warfarin and aspirin. In 2024, after warfarin discontinuation, a recurrent inferior STEMI occurred, treated with percutaneous transluminal coronary angioplasty (PTCA) and thromboaspiration of the distal RCA. The patient was discharged on warfarin and clopidogrel. Warfarin was later replaced with rivaroxaban, leading to another episode of inferior non-ST-elevation myocardial infarction (NSTEMI). Angiography demonstrated a markedly aneurysmal RCA with slow flow and critical proximal stenosis. PTCA or stent implantation was deferred due to the absence of suitable device sizes and the patient was discharged with warfarin lifelong indication. Discussion: CAE is a rare condition, observed in 0.3–5% of patients undergoing coronary angiography. In adults, the most common cause is atherosclerosis, followed by connective tissue diseases, rheumatologic conditions, and infections. Angiography remains the gold standard for assessing the location, size, and morphology of the aneurysm. This clinical case underscores the therapeutic complexity of coronary ectasia. Invasive and surgical options remain technically challenging and individualized and may include balloon angioplasty, implantation of covered stents, coil embolization for peripheral saccular aneurysms, or, in rare cases, surgical resection of the aneurysm. While medical therapy continues to rely on expert opinion. Long-term anticoagulation may represent the cornerstone of secondary prevention in patients with recurrent thrombotic events and flow disturbances related to coronary ectasia.