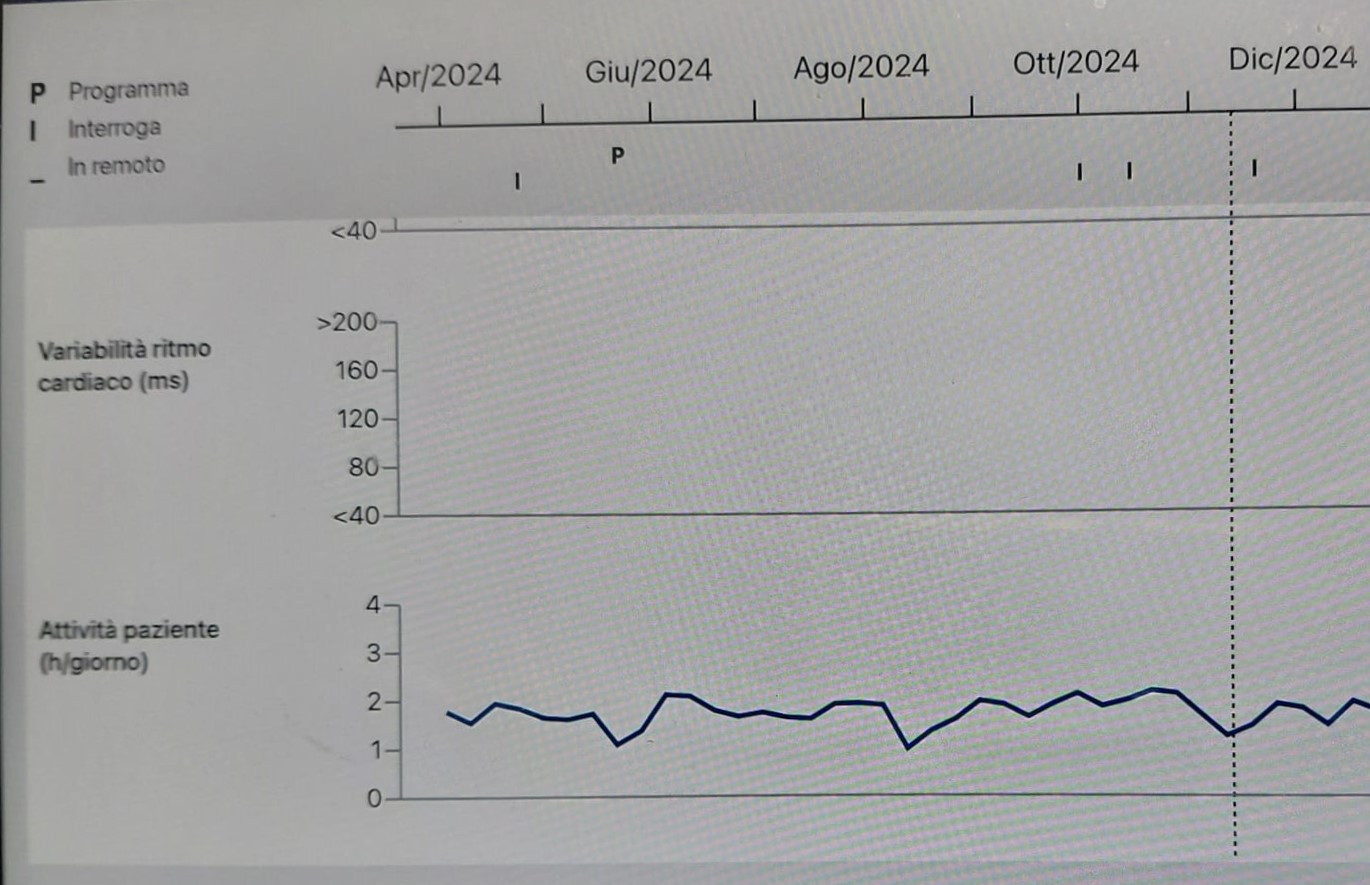
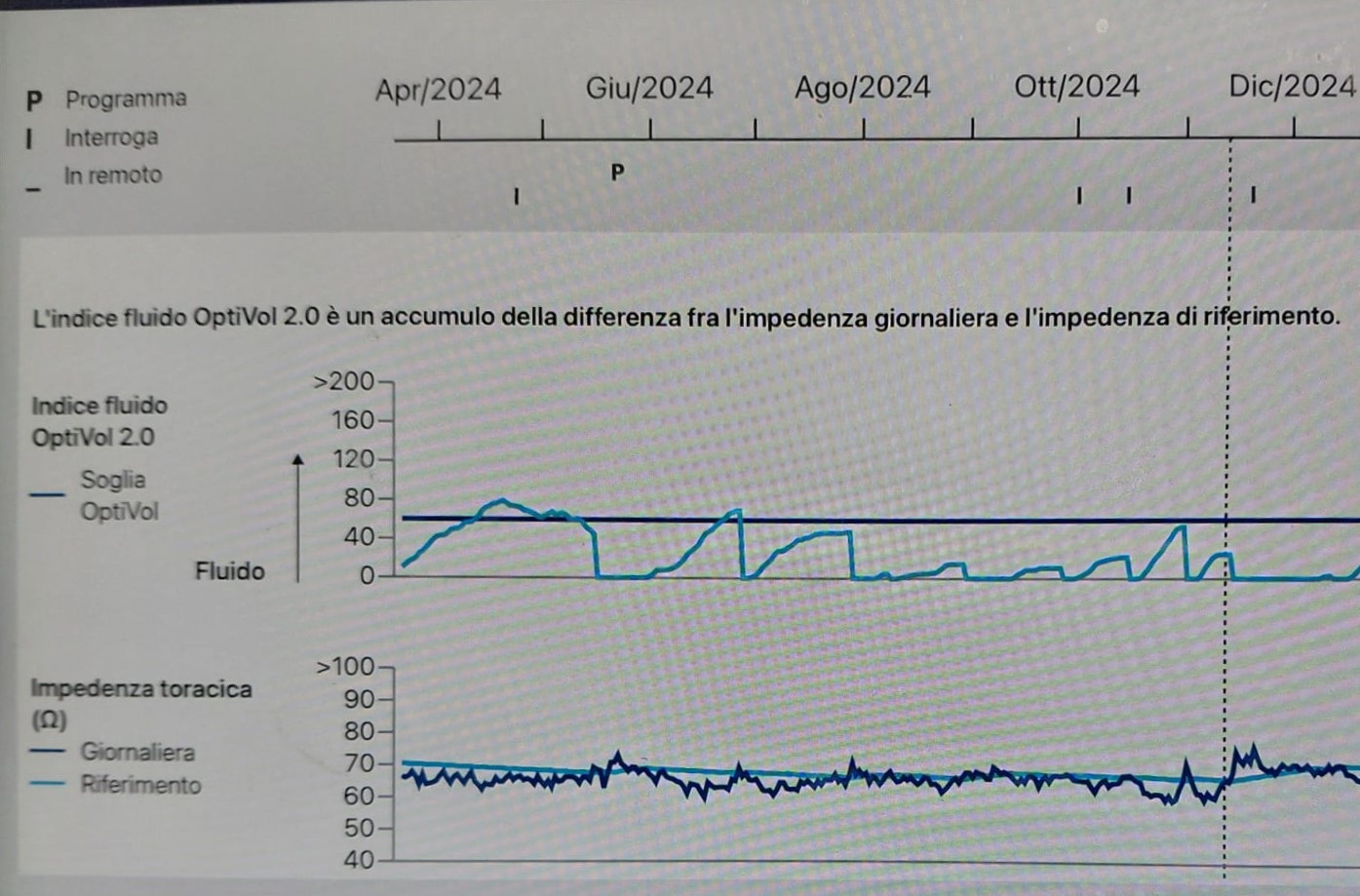
A 72-year-old female patient with non-ischemic dilated cardiomyopathy (FE 30%) presented to our attention due to persistent dyspnea, despite optimized medical therapy for heart failure. In particular, her medication regimen included: sacubitril/valsartan 49/51 x2/die, dapagliflozin 10 mg/die, bisoprolol 7.5 mg/die, furosemide 25 mg/die, and vericiguat 10 mg/die (the latter for 6 months). Her medical history included: a dual-chamber defibrillator (Medtronic) implantation in 2023 and permanent atrial fibrillation with a narrow QRS complex (90 ms). Given her symptoms and clinical hystory, cardiac contractility modulation (CCM) therapy was proposed and implanted contralaterally to the defibrillator, thus on the right side. Both the procedure and hospital stay were uneventful, and the patient was discharged. Subsequent follow-ups were conducted at 1 month and 6 months with clinical cardiological evaluation, device checks of the defibrillator and CCM, echocardiogram, and the Minnesota Living with Heart Failure Questionnaire (MLHFQ). The echocardiogram showed no significant signs of improvement at 6 months. The initial MLHFQ score was 60. It remained unchanged at 1 month, but at 6 months a significant improvement was registered with a score of 40. The patient reported a subjective improvement in quality of life, with reduced dyspnea during certain daily activities and no longer required diuretic/furosemide therapy. AICD monitoring, however, revealed an interesting trend in the diagnostic parameters collected daily by the device and grouped in trends (Compass Medtronic). In particular there was not a significant improvement in daily hourly activity, but a marked improvement in the amount of intracorporeal fluid (OptiVol) and a reduction in the percentage of daily ventricular pacing. Discussion: CCM therapy is a valid alternative in patients with symptomatic heart failure to reduce hospitalizations when optimized therapy is not sufficient. In the discussed case, the device ensured an improvement in symptoms, probably in daily activities with lower energy expenditure, and significantly reduced congestion (demonstrated not only by improved OptiVol values, but also by enabling discontinuation of the diuretic). Evaluating the diagnostic tools available from continuous device monitoring could be an even more objective parameter to validate the effectiveness of CCM, in contrast to the NYHA and MLHFQ, which instead represent more subjective evaluation systems.