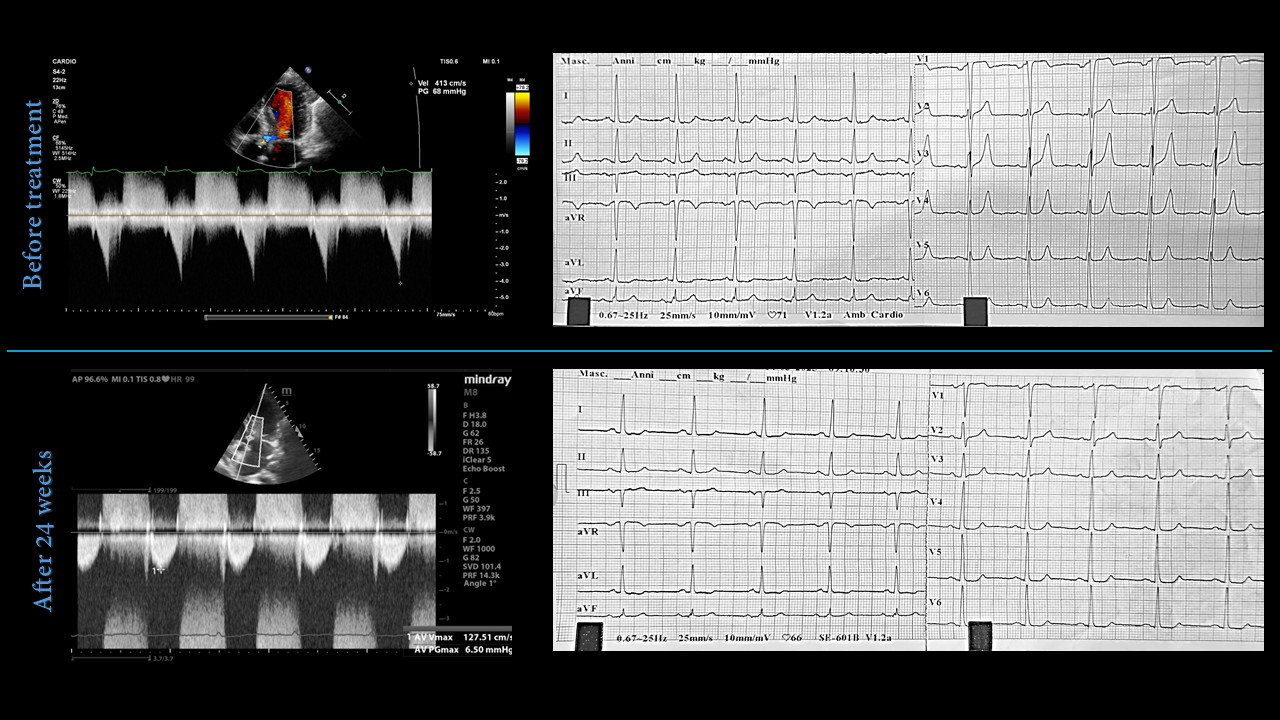
In November 2023, a 38-year-old woman was referred to our outpatient clinic for dyspnea. Her medical history included systemic lupus erythematosus complicated by lupus nephritis for which she underwent renal transplantation in 2017. She was in NYHA class III with signs of congestive heart failure. Electrocardiography showed sinus rhythm at 70 bpm with normal atrioventricular and intraventricular conduction, high voltages, and repolarization abnormalities consistent with left ventricular hypertrophy. Transthoracic echocardiography demonstrated asymmetric hypertrophy, left ventricular outflow tract (LVOT) obstruction with a resting gradient of 68 mmHg, increasing to 95 mmHg with Valsalva manoeuvre, left ventricular ejection fraction (LVEF) of 60% and preserved right ventricular systolic function. Cardiac magnetic resonance confirmed asymmetric septal hypertrophy (maximal wall thickness of 18 mm) and diffuse interstitial fibrosis with non-ischemic late gadolinium enhancement in inferolateral, inferior, anterolateral and apical segments. Metoprolol was initiated and later combined with disopyramide, which was soon discontinued due to gastrointestinal intolerance. Mavacamten therapy was initiated at 5 mg daily. After four weeks, the patient reported symptomatic improvement, although LVOT gradients remained unaltered. At week 12, the dose was increased to 10 mg daily. Four weeks later, the patient was in NYHA class II, with complete resolution of LVOT obstruction and a slight reduction in interventricular septal wall thickness (16 mm vs 18 mm). From treatment initiation, a reduction in ECG voltages was observed, with a 13 mm decrease in the Sokolow-Lyon index, alongside a marked reduction in NT-proBNP (973 pg/ml vs. 5000 pg/ml at baseline). At 30 weeks genetic testing revealed an heterozygous PTPN11 mutation (c.184T>A, p.Tyr62Asn, Class 4) consistent with Noonan syndrome. At 60 weeks the patient remained stable in NYHA class II with a preserved LVEF. Conclusion. This case illustrates the clinical and structural effects of mavacamten in a patient with obstructive hypertrophic cardiomyopathy ultimately linked to Noonan syndrome. In this patient, mavacamten provided symptomatic relief, resolution of LVOT obstruction, initial signs of structural remodelling and a substantial reduction in NT-proBNP, suggesting – despite its unselective mechanism of action – meaningful benefit in this complex setting.