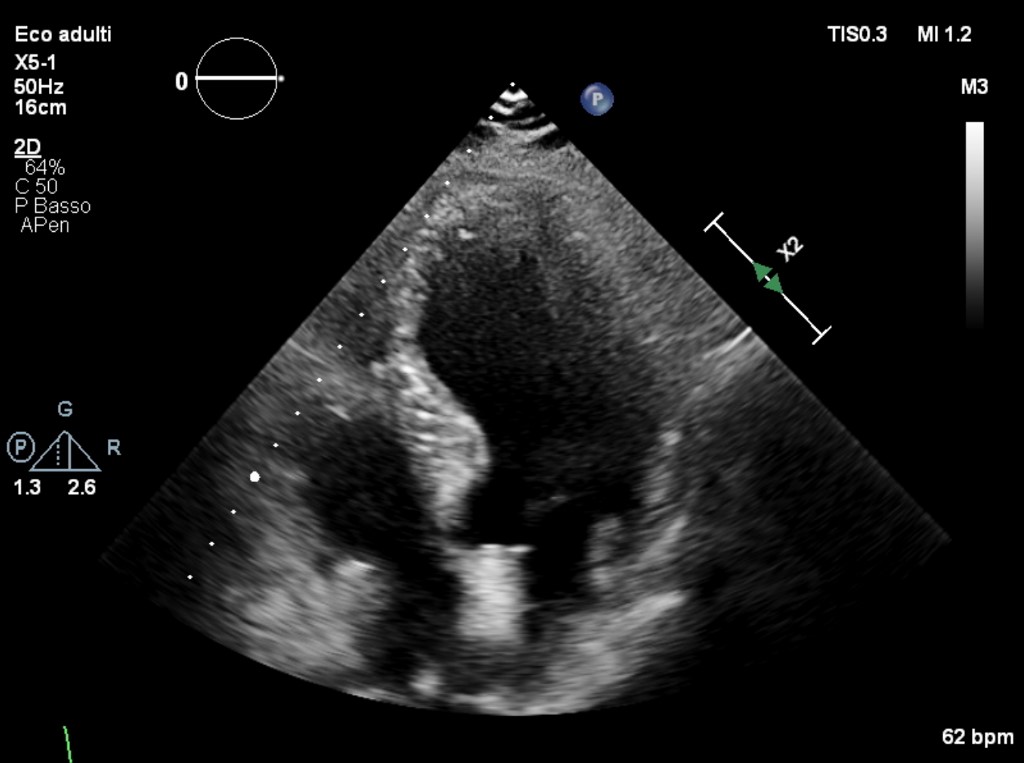
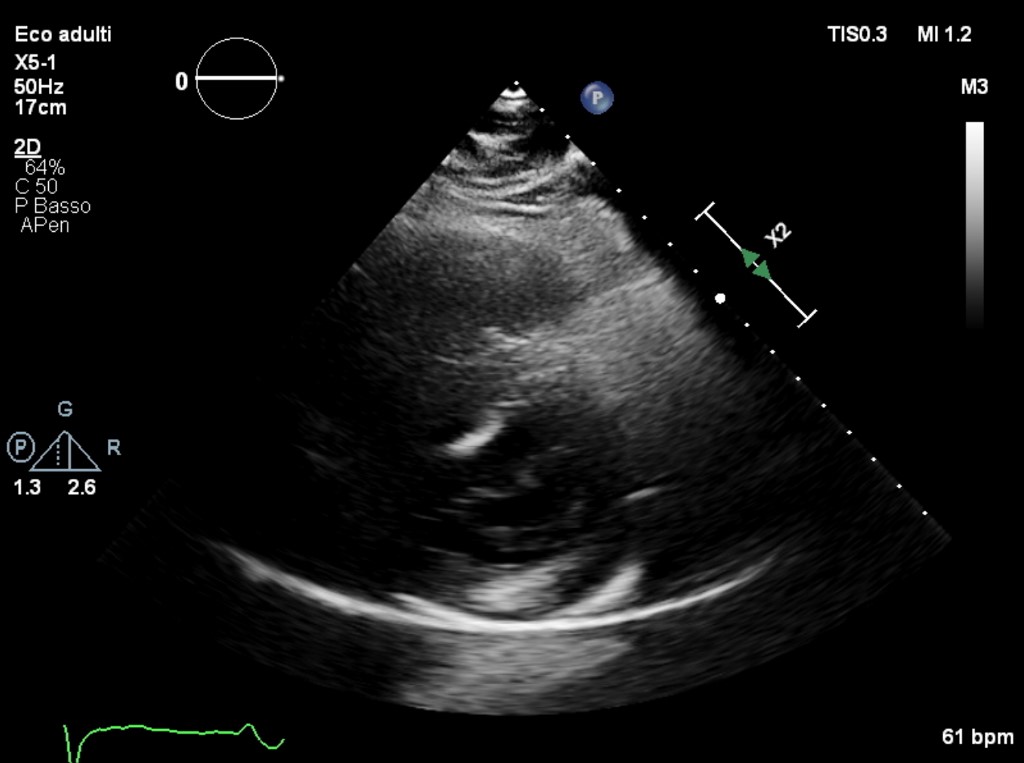
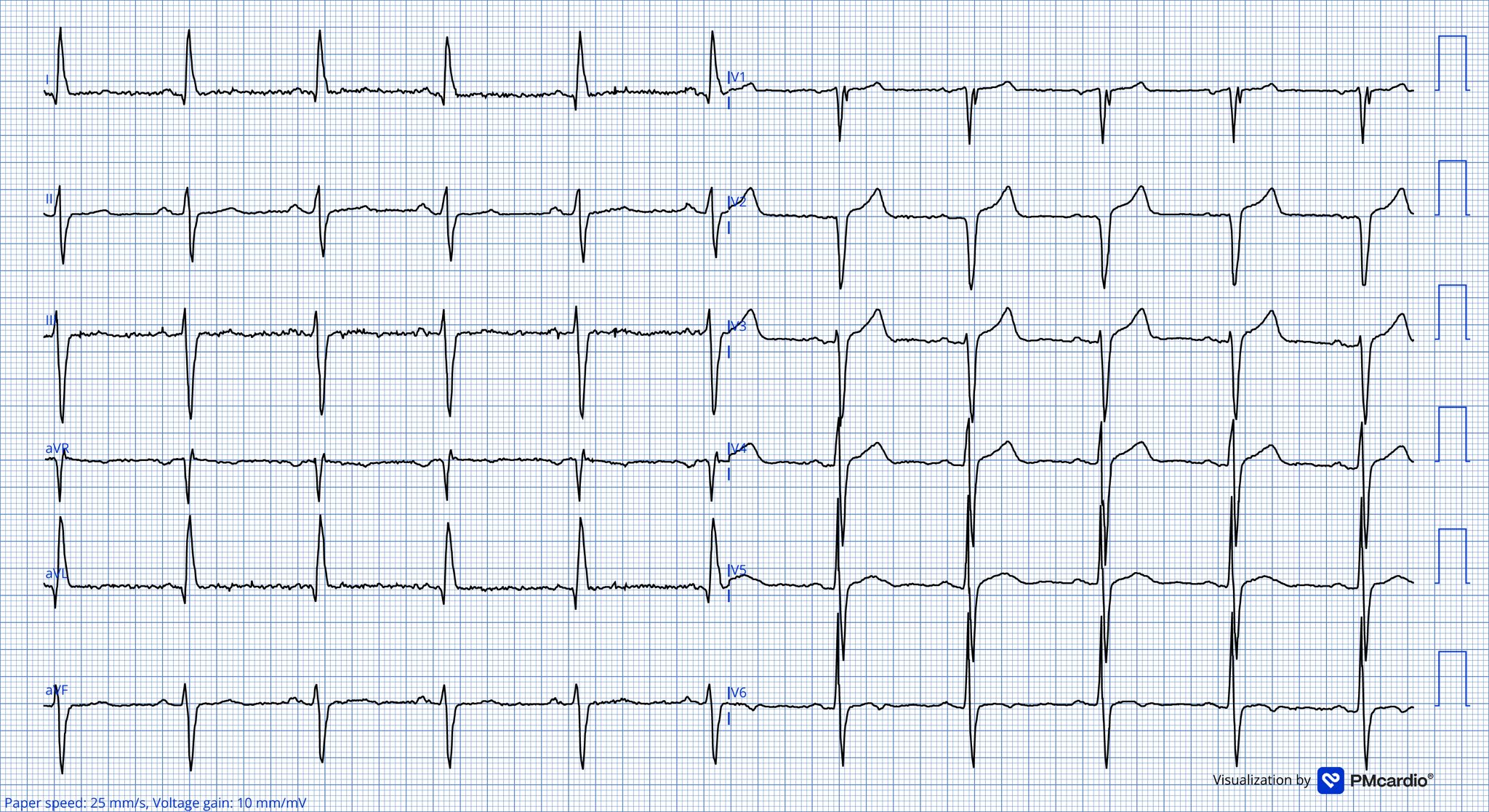
Background: Fabry disease may present with a late-onset phenotype and predominantly cardiac involvement; diagnosis can emerge through cascade screening even in asymptomatic individuals. Case presentation: A 70-year-old man was referred after Fabry disease was identified through family screening triggered by a positive newborn screening result in a second-degree grandchild. Pedigree-based cascade screening subsequently led to the diagnosis in one of his daughters and two grandchildren. The patient denied cardiac symptoms (angina/equivalents, palpitations, syncope, or dyspnea). Past medical history was notable only for parkinsonism on medical therapy; no cardiovascular risk factors were present. ECG showed sinus rhythm with right bundle branch block and left anterior fascicular block; T-wave inversion in V6 and flattened T waves in the inferior leads. Transthoracic echocardiography demonstrated normal left ventricular volumes and preserved global systolic function, with focal hypokinesia of the posterior wall and a hyperechogenic area in the basal posterior segment extending to the adjacent inferior wall. Right ventricular size and function were normal. Mild aortic, mitral, and tricuspid regurgitation were observed. There were no signs of congestion and no pericardial effusion. Biochemical/genetic testing revealed markedly reduced alpha-galactosidase A activity on dried blood spot (0.4 nmol/mL/h) and elevated lyso-Gb3 (18 nmol/L); genetic analysis identified the GLA variant c.337T>C (p.Phe113Leu). Enzyme replacement therapy was initiated (biweekly infusions). The patient reported a recurrent improvement in overall well-being during the first 10 days following each infusion; lyso-Gb3 was decreasing on follow-up assessments. Cardiac MRI is scheduled; the patient undergoes semiannual cardiology follow-up with renal function monitoring. Discussion/Conclusions: The GLA c.337T>C variant has been associated with a late-onset phenotype with predominant cardiac involvement and has been described in familial clusters. The focal infero-posterior hyperechogenic echocardiographic finding may be consistent with tissue changes reported in Fabry cardiomyopathy, but it is not pathognomonic and requires confirmation/staging by cardiac MRI. This case highlights the value of cascade screening to detect early, paucisymptomatic cardiac involvement. The co-existence of parkinsonism, while not proving causality, may represent an area for future research.