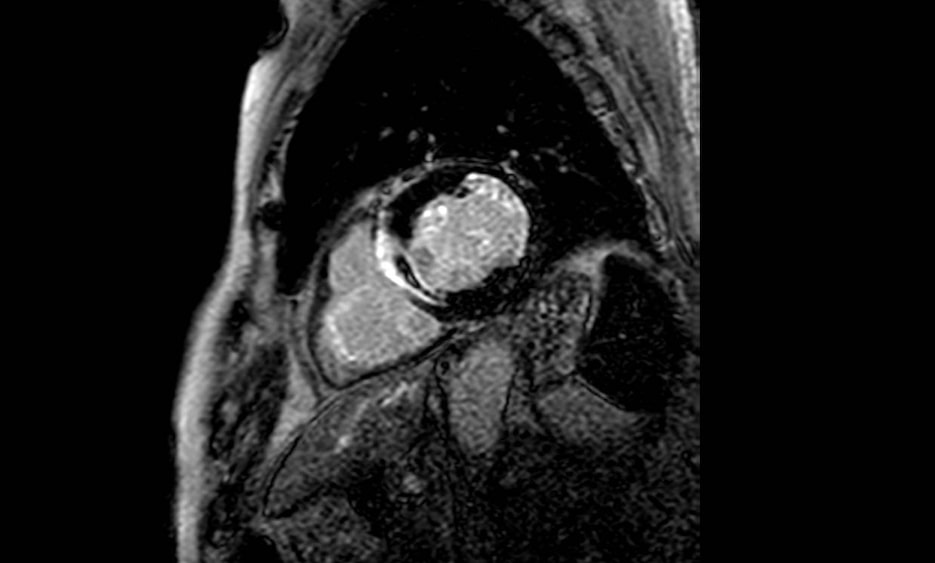
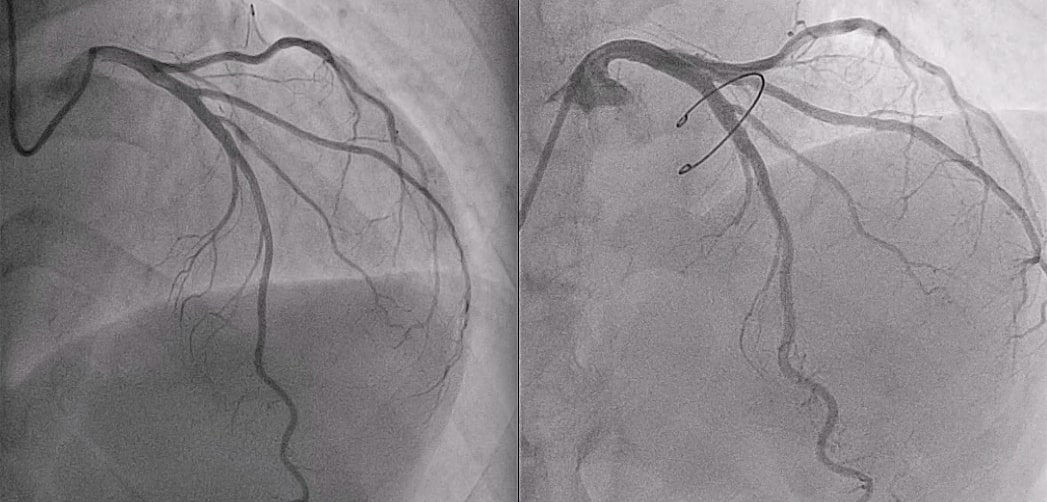
Patients with ACS and unobstructed coronary arteries represent a clinical dilemma and their diagnosis and management is quite variable in current practice. A 69-year-old man, who underwent valvuloplasty in 2013 for severe mitral regurgitation, presents with troponin-positive typical chest pain and a newly diagnosed RBBB that is identified as suspicious for NSTE-ACS. Coronary angiography reveals a critical ostial stenosis of the intermediate branch of the LCA with preserved TIMI flow. Since there are no other coronary lesions, conservative treatment is chosen. In the following days diarrheal attacks and an increase in inflammation markers is reported. TTE shows a slightly reduced LVEF with hypokinesia of the basal segments of the infero-posterior wall and of the lower IVS. The patient was discharged with a diagnosis of suspected acute myocarditis complicated by mild left ventricular dysfunction. After one month, cardiac MRI is performed with evidence on one hand of akinesia and thinning of mid-basal infero-lateral wall with transmural LGE extended to the posterior papillary muscle (indicating a previous MI); on the other hand of akinesia of the basal septum with transmural LGE and signs of microcirculatory obstruction (MVO) and acute inflammation on T2-weighted sequences (indicating a recent MI). Moderate left ventricular systolic dysfunction (EF 36%) is highlighted. The MRI performed after 6 months confirms ischemic dilated cardiopathy with moderate left ventricular dysfunction. Following these findings, the coronary angiography is re-evaluated and compared with that of 2013 with evidence in the last study of an occlusion of the first septal branch of the LCA and a distortion in the course of the circumflex branch compared to the previous exam. What about the etiology of these unrecognized myocardial infarctions? Could the previous lateral infarction be the results of distortion in the circumflex branch’ s course caused by surgical sutures of mitral valvuloplasty? Could the septal branch closure causing the new septal infarction have occurred due to an extra-coronary embolic event? Accurate diagnosis of the underlying patho-physiological mechanisms leading to the troponin rise is surely important for initiation of appropriate treatment, but may also have long-term implications for the patient. CMR and its unique non-invasive myocardial tissue characterization do not just have a diagnostic role but it has a potential role in risk stratification.