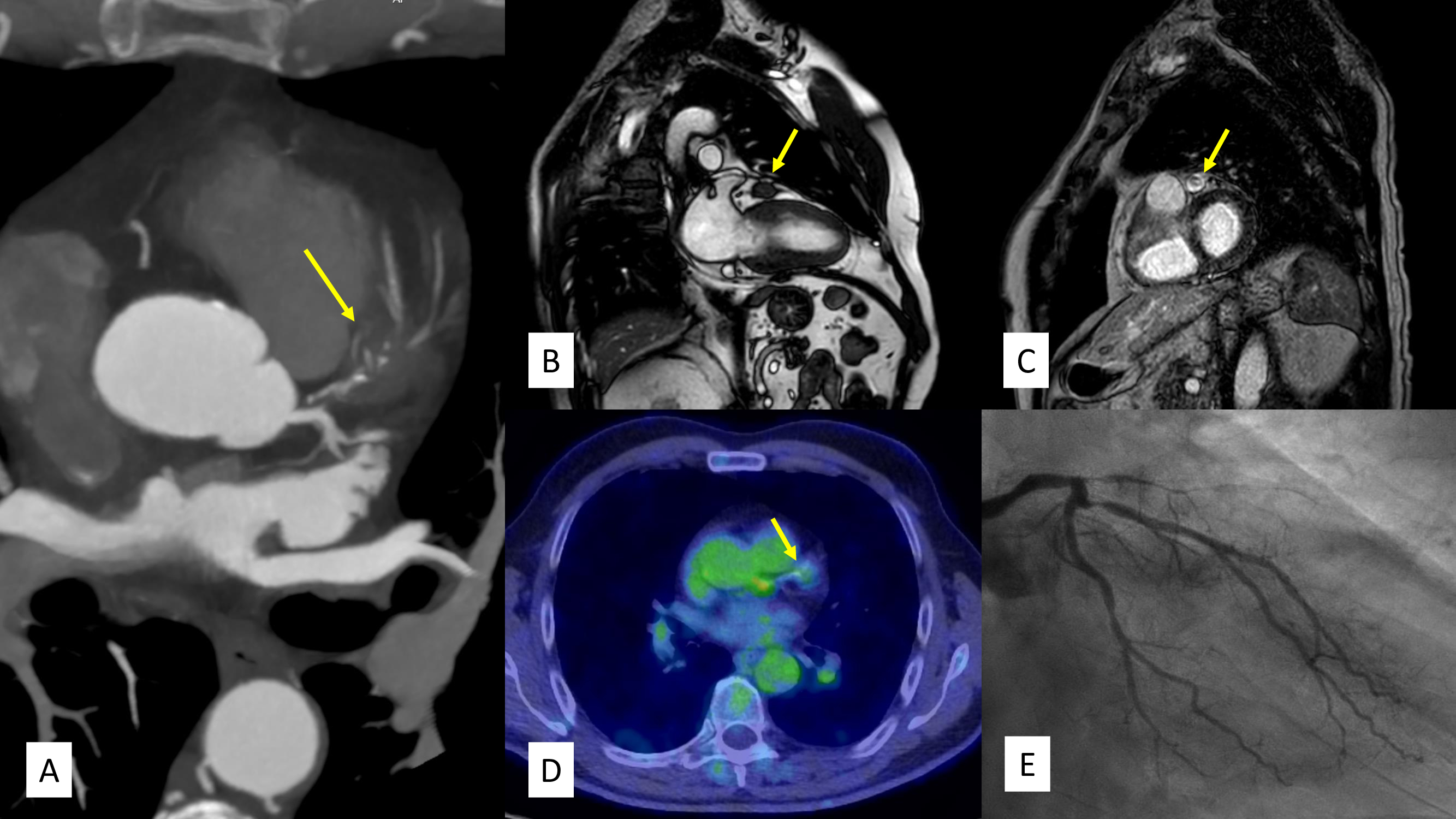
A 71-years-old man with typical chest pain and a stress test positive for angina with negative ECG criteria underwent coronary computed tomography angiography (CCTA) which detected a chronic total occlusion (CTO) in the proximal-mid segment of the left anterior descending artery (LAD). Notably, the proximal tract of LAD was compressed by a hypodense oval solid lesion with mild late enhancement (Panel A). Cardiac magnetic resonance imaging (MRI) confirmed the presence of solid tissue approximately 2 x 1.5 cm in size (Panel B), characterized by a hypodense appearance on T2 and STIR sequences, with no significant restriction of diffusivity but hyperintense on intermediate b-value sequences, suggestive of moderate cellularity, and with marked late gadolinium enhancement (LGE) (Panel C); 18-FDG-PET, was negative for any cardiac lesions with significant uptake (Panel D). Finally, coronary angiography (Panel E) confirmed the anatomical data obtained through CCTA and also revealed a critical stenosis of the obtuse marginal branch (MO) of the circumflex artery. The primary hypothesis is that the tissue is fibrotic, possibly resulting from a localized histiocytosis, in the absence of other systemic disease involvement. Other differential diagnoses include primitive stromal lesions such as fibroma and low-grade fibrosarcoma, angiosarcoma and IgG4-related disease. The case was discussed collegially in a Heart Team meeting, with cardiothoracic surgeon, oncologist and radiologist. Considering the limited territory of distribution of the LAD (also suggested by the stress test positive for angina but negative for ECG criteria), and the presence of radiological findings consistent with a low-grade mesenchymal neoplasm, the decision was to proceed with optimal medical therapy and percutaneous coronary intervention (PCI) on MO, active surveillance and to consider re-evaluation for bypass grafting and lesion biopsy in the event of further disease progression.