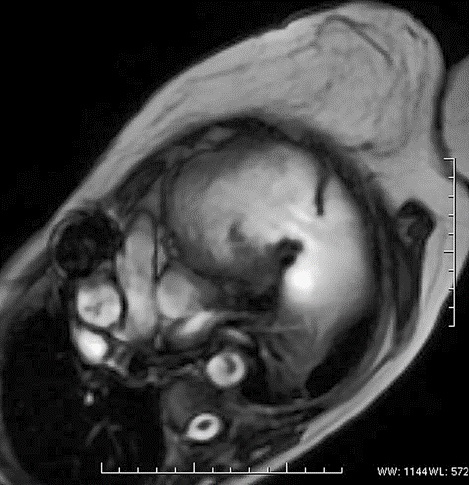
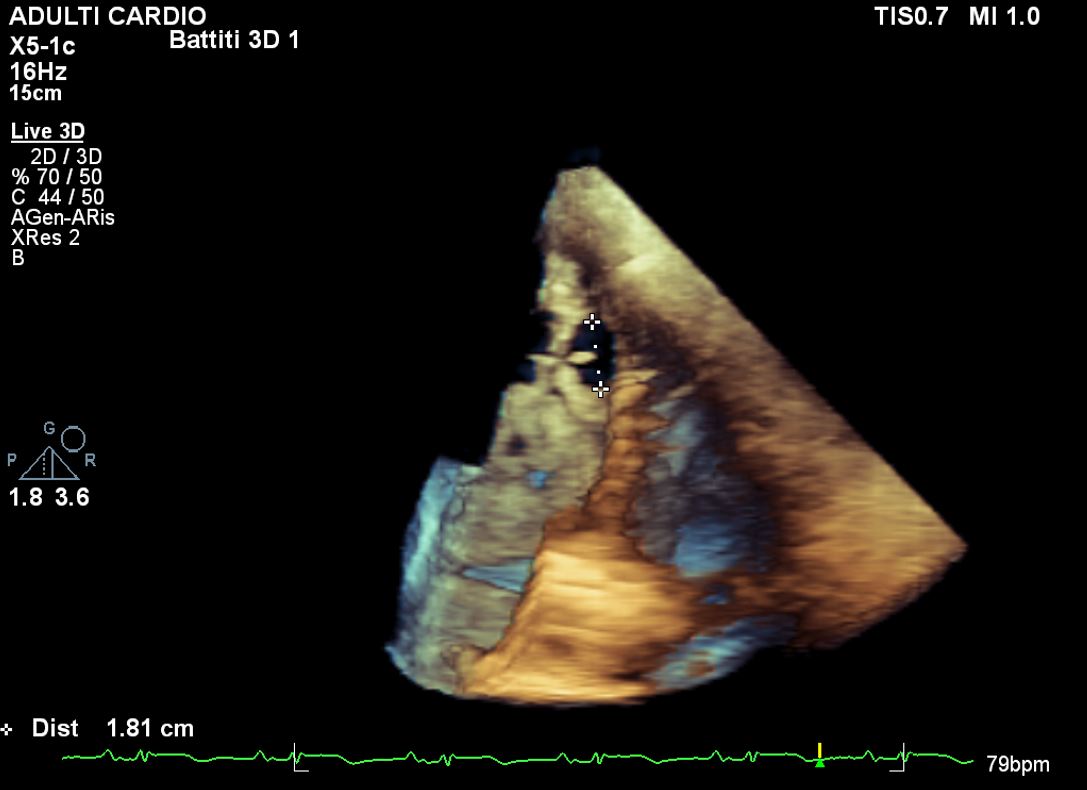
Background: Takotsubo Syndrome (TTS) is characterized by transient, reversible left ventricular dysfunction, often triggered by severe physical or emotional stress, leading to secondary catecholaminergic hyperactivation. It occurs without significant coronary artery obstruction. Although TTS is usually benign, it can be complicated by severe conditions like left ventricular wall rupture, which occurs in less than 1% of cases. This report presents the case of a patient with TTS who developed left ventricular wall rupture and subsequent complications. Case Report: A 57-year-old woman with no significant medical history was admitted in February 2022 for TTS complicated by left ventricular free wall rupture. Coronary angiography revealed no significant coronary lesions, with only 40% stenosis in the second obtuse marginal branch (OM2). After stabilization, the patient underwent surgical repair using a triple-layer patch. Upon discharge, transthoracic echocardiography showed a left ventricular end-diastolic volume of 167 mL, an ejection fraction (EF) of 35%, and normal right ventricular function. Cardiac MRI revealed severe left ventricular dilation and dysfunction following inferolateral wall repair. Regular cardiology follow-ups showed no significant changes. In September 2024, the patient reported reduced exercise tolerance (NYHA class IIb) and was referred to ISMETT for advanced therapies. Elective cardiac MRI revealed severe left ventricular dilation, significant systolic dysfunction, and a large pseudoaneurysmal cavity communicating with the left ventricle. Ischemic-pattern enhancement was noted in the left coronary artery distribution. Coronary angiography showed critical stenosis in the mid and distal segments of the OM1 with a reduced vessel diameter. In November 2024, the patient underwent surgical correction of the left ventricular pseudoaneurysm, with reconstruction of the posterolateral ventricular wall using a Dacron patch. Postoperative recovery was uneventful, with extubation on the first day and transfer from ICU to the ward. She remained clinically stable throughout the hospital stay. A postoperative echocardiogram showed severe left ventricular dilation and dysfunction (EF 27%) after pseudoaneurysm exclusion and patch repair, mild-to-moderate mitral regurgitation, normal right ventricular function, and normal pulmonary artery pressures. The patient was transferred to a rehabilitation facility to continue her physical therapy.