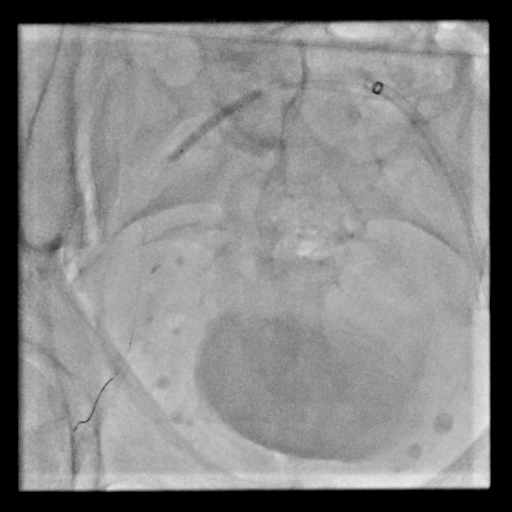
Background. Catheter ablation for atrial fibrillation (AF) is technically demanding, and vascular access complications remain among the most frequent and clinically important adverse events. Although ultrasound-guided femoral puncture has improved safety, multiple venous punctures, large-bore sheaths, and full anticoagulation mean that rare, potentially life-threatening complications can still occur. Case Description. A 69-year-old man with ischemic dilated cardiomyopathy and a prior implantable cardioverter-defibrillator (ICD) was referred for pulsed-field ablation (PFA) for symptomatic AF refractory to maximal medical therapy, with recurrent inappropriate ICD shocks. During acquisition of dual right femoral venous access under ultrasound guidance, a 7-French introducer sheath kinked and ruptured after contact with an advancing SL0 long sheath. Venography confirmed retention of the distal fragment in the right femoral vein. A multidisciplinary team, including an interventional radiologist and a vascular surgeon, was promptly activated, and an endovascular-first retrieval was pursued via contralateral femoral access. After unsuccessful gooseneck snare attempts, balloon-assisted retrieval was performed: an 8-French Cook sheath was advanced from the left femoral vein; a 4-French Berenstein catheter with a 0.035″ guidewire engaged the fragment lumen; ( Fig.1 ) the 0.035″ wire was exchanged for a 0.014″ wire and the catheter for a 4.0 × 30-mm semi-compliant balloon, advanced into the fragment, inflated, ( Fig.2 ) and used to pull it to the left femoral vein for controlled extraction ( Fig.3 ). Final venography demonstrated preserved bilateral venous integrity. PFA was then completed uneventfully through the remaining secure accesses, achieving complete pulmonary vein isolation. At three-month follow-up, the patient remained in sinus rhythm without arrhythmic events or vascular sequelae. Conclusions. This case illustrates an uncommon but high-risk access complication—introducer sheath rupture with intravascular fragment retention—despite ultrasound guidance. Rapid recognition, venographic confirmation, and multidisciplinary involvement enabled a conservative endovascular strategy, avoiding open venous exploration. Early diagnosis and coordinated management are essential. When feasible, an endovascular-first approach—using balloon-assisted techniques when snaring fails—can be safe and effective, preserving venous integrity.