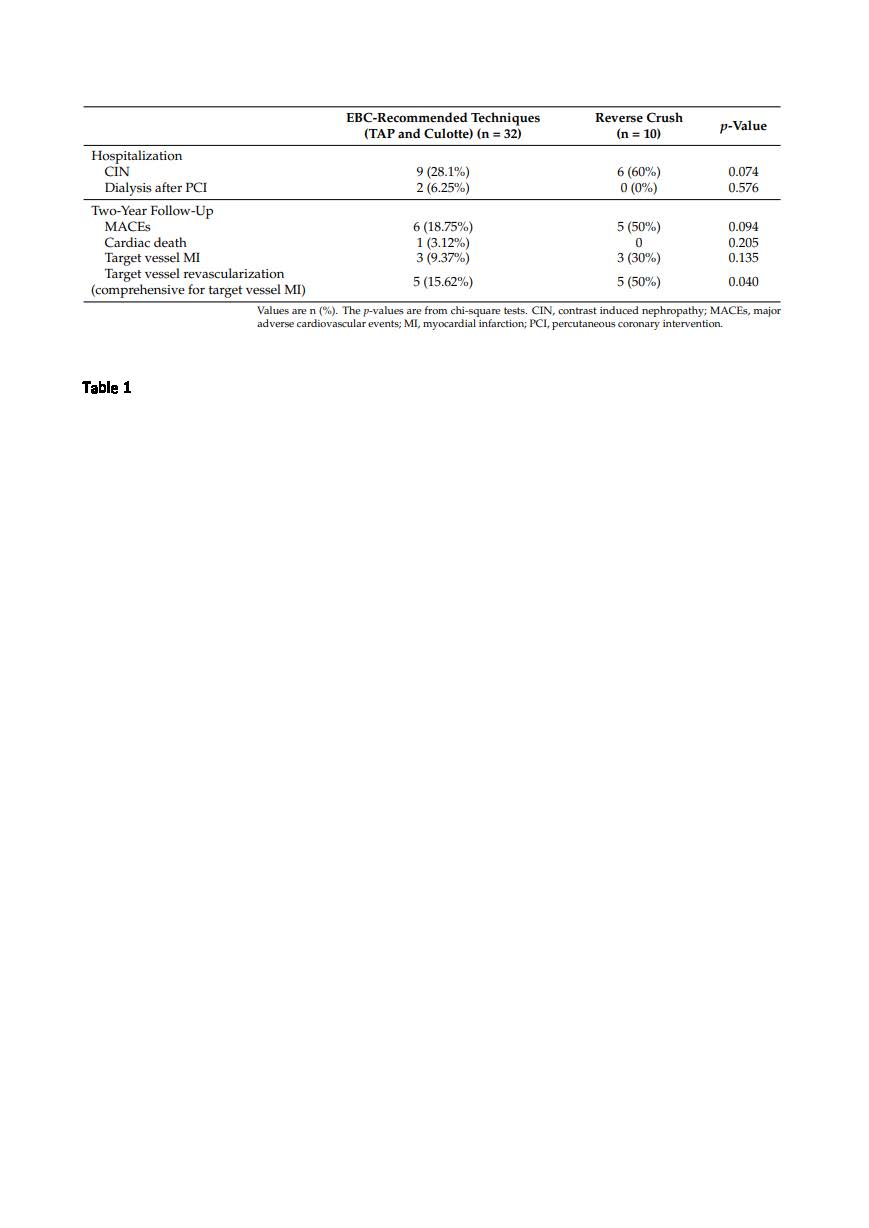
In the event of failure of a provisional approach for treatment of coronary bifurcation lesions, many two-stent bifurcation techniques can be performed. Two techniques (culotte and T/TAP) are suggested by the European Bifurcation Club, but a reverse crush is performed by some operators. This study aims to retrospectively compare these two different approaches (EBC-recommended techniques vs. reverse crush). The primary endpoint was MACEs during two years of follow-up. This was a retrospective study. There was a high prevalence of type 2 diabetes mellitus (31%). The most common admission presentation was NSTEMI (69%). There were no significant differences in age, sex, comorbidities, or presentation type between the two comparison groups. The most treated coronary bifurcation was the left main (64.28%), followed by the left anterior descending artery–first diagonal (33.33%). The predominant lesion type was Medina 1.1.1 (88.1%). A significant proportion of the treated bifurcation lesions were classified as complex according to the Definition Criteria (42.85%) and 38.09% were severely calcified (angiographic assessment). The side branch lesion length was longer than 10 mm in many cases (69%). The side branch stenosis was severe in 85.71%. A high SYNTAX score > 32 was present in 30.95%. Regarding the baseline angiographic characteristics, the two comparison groups differed significantly only for the presence of more patients with a high SYNTAX score (>32) in the reverse crush group. During the follow-up, six patients experienced a target vessel acute myocardial infarction (14.28%), often caused by thrombosis at the ostium of the side branch or at the distal edge of previously implanted stents. In total, at 24 months, 10 patients underwent target vessel revascularization (23.81%) and only one patient died (due to an acute pulmonary edema related to a suspected acute myocardial infarction). At two years follow-up, EBC-recommended techniques were significantly associated with a lower incidence of target vessel revascularization (9.37% vs. 30%, p-value = 0.040) compared with the reverse crush group; in the EBC group, there was also a trend toward a lower incidence of CIN after the PCI, but it was not statistically significant (28.1% vs. 60%; p-value = 0.074), and a lower incidence of MACEs was found (18.75% vs. 50%, p-value = 0.094). EBC-recommended techniques should be preferred to reverse crush even if this study ha numerous limitations.