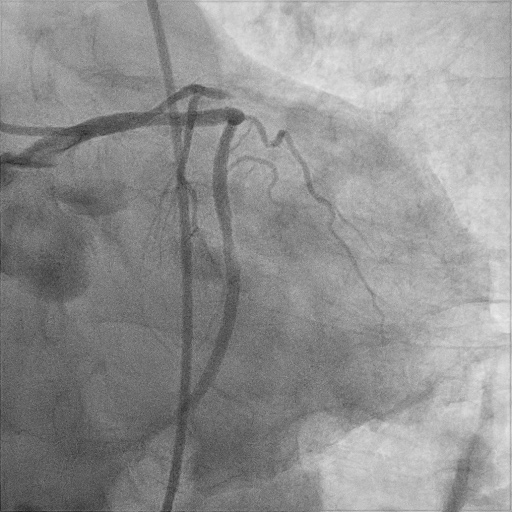
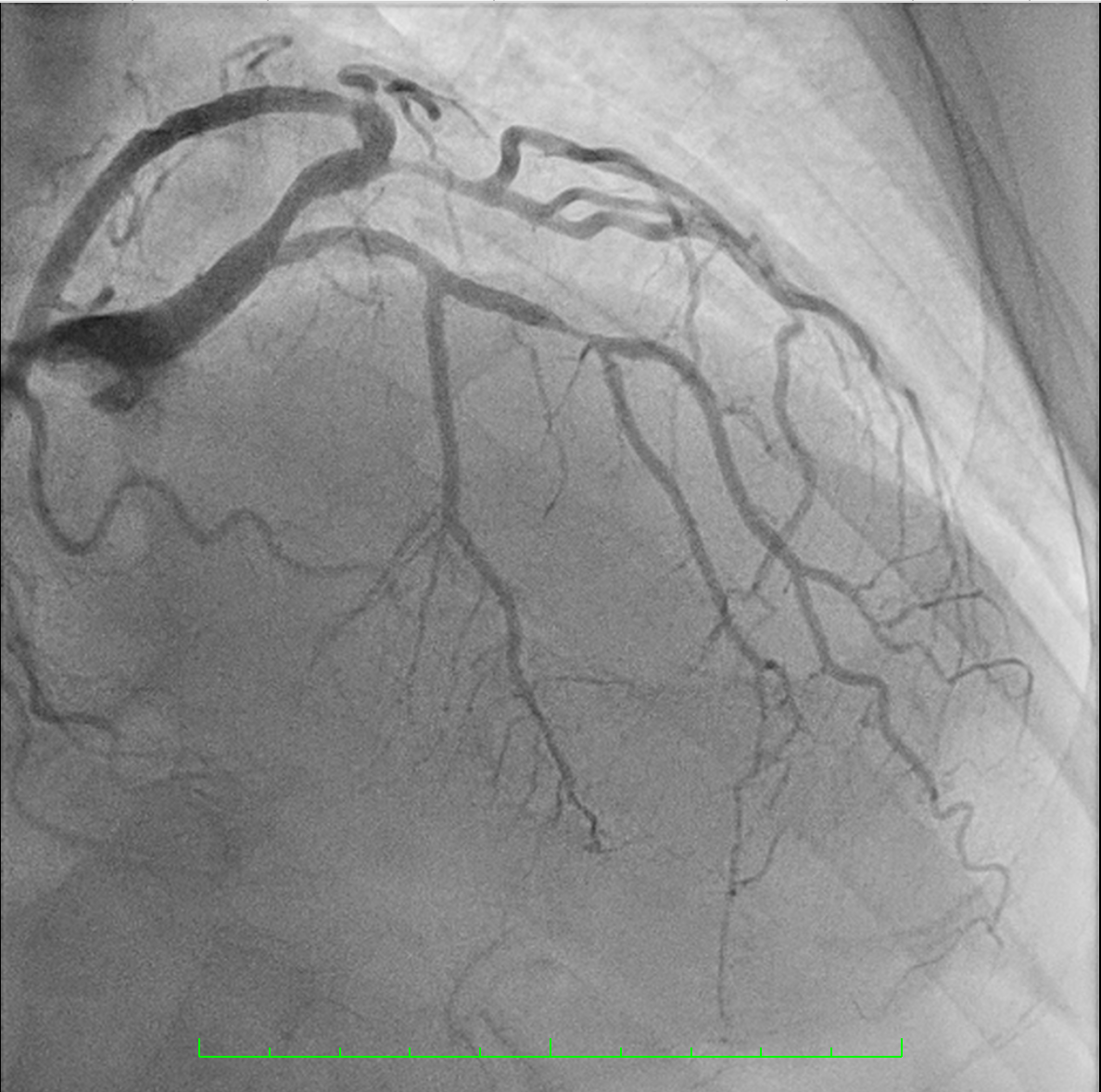
Background: Drug-coated balloon (DCB)–only percutaneous coronary intervention (PCI) represents a “leave-nothing-behind” strategy that may allow very-short dual antiplatelet therapy (DAPT), an appealing option in high-bleeding-risk patients requiring urgent non-cardiac surgery. However, acute vessel occlusion following DCB treatment of de-novo lesions remains an uncommon but potentially catastrophic complication. Case summary: A 73-year-old man with prostate cancer awaiting urgent surgery underwent coronary evaluation, which revealed sub-occlusive stenoses of the mid–left anterior descending artery (LAD) and the proximal first obtuse marginal branch (OM1). To minimize DAPT duration, a DCB-only strategy was selected. After lesion preparation with semi-compliant balloons, both vessels were treated with paclitaxel-coated balloons, achieving an apparently optimal angiographic result without visible dissection. Fifteen minutes after leaving the catheterization laboratory, the patient developed chest pain, hypotension, and anterolateral ST-segment elevation. Urgent repeat angiography demonstrated acute thrombotic occlusion of the LAD and sub-occlusion of OM1 at the treated segments. Bail-out drug-eluting stent implantation restored coronary flow with rapid clinical stabilization. Conclusion: This case highlights that acute vessel occlusion may occur very early after DCB-only PCI despite angiographic success, particularly in complex de-novo lesions. Rigorous lesion preparation, careful patient and lesion selection, consideration of intracoronary imaging, and preparedness for immediate bail-out stenting are essential when adopting a stent-free strategy in patients requiring ultra-short DAPT.