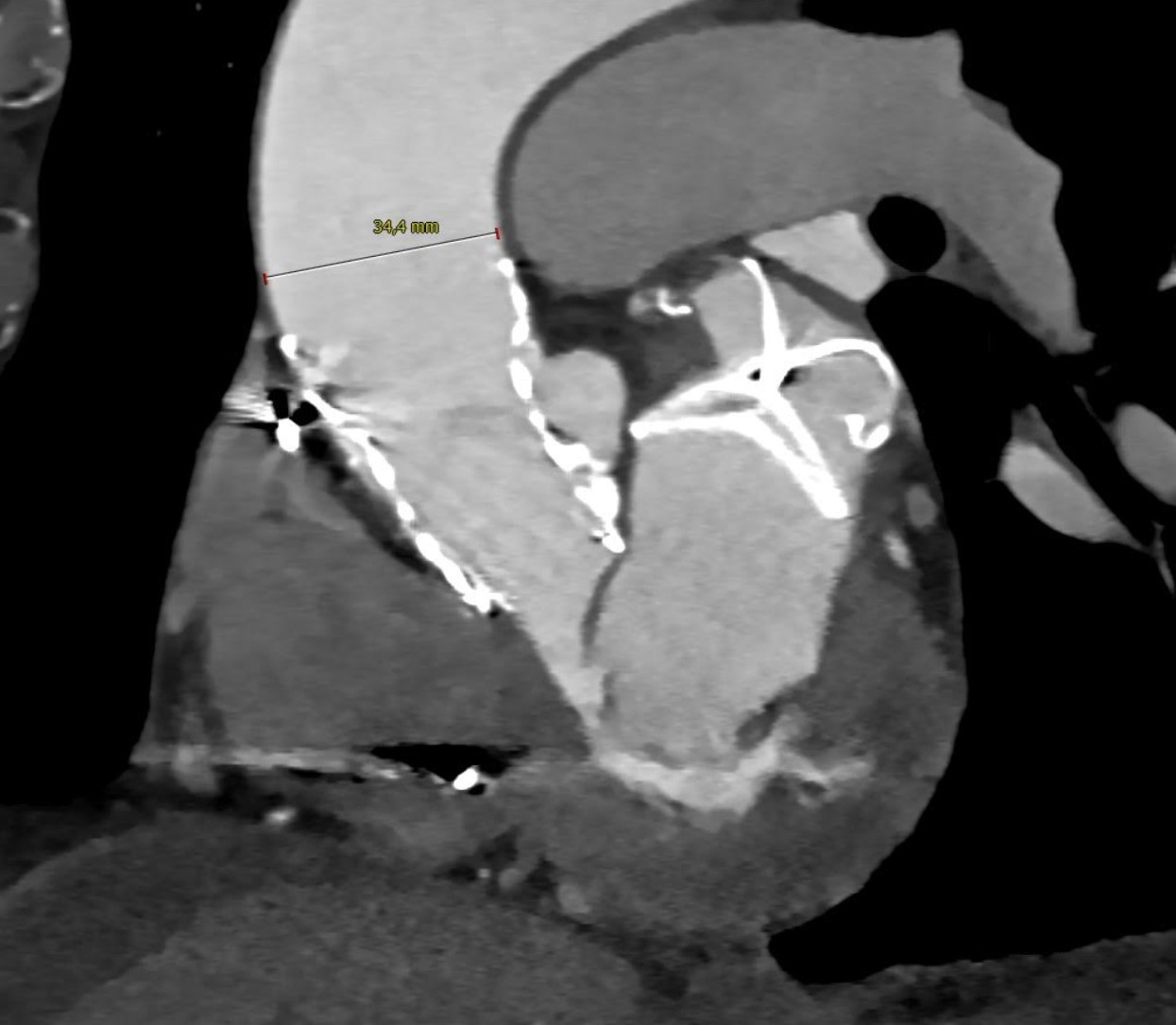
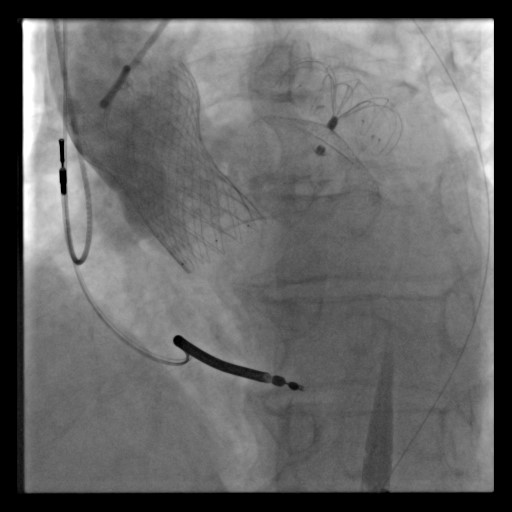
An 80-year-old male with multiple comorbidities (Charlson Comorbidity Index: 14), including paroxysmal atrial fibrillation, HFmrEF (NYHA III), cardiac amyloidosis due to multiple myeloma, transvenous ICD for primary prevention, COPD, multifactorial anemia, thrombocytopenia, advanced chronic liver disease with recurrent esophagogastric variceal hemorrhage (F3 varices), and CKD (KDIGO G3b), presented with low-flow, low-gradient severe aortic stenosis (Gmax/mean 42/22 mmHg; LVOTd 23 mm; AVA-VTI 0.9 cm²). The patient’s surgical risk was high (EUROSCORE II of 17.72%). Due to recurrent bleeding, anticoagulation was contraindicated, necessitating both left atrial appendage occlusion (LAAO) and transcatheter aortic valve implantation (TAVI). LAAO was performed using a 36 mm LAmbre device under conscious sedation. Intracardiac echocardiography (ICE) was used instead of TEE to eliminate the need for intubation and reduce the risk of variceal bleeding. An 8F transseptal introducer was inserted into the superior vena cava, followed by transseptal puncture. An Amplatzer Superstiff guidewire was advanced into the left superior pulmonary vein, and a 10F delivery sheath was advanced over the guide. The sheath was advanced into the LAA using a 6F pigtail catheter, followed by sizing of the landing zone. The LAAC device was implanted with good results. The patient then underwent TAVI with a self-expanding 34 mm Evolut FX bioprosthesis. The anesthesiological protocol included induction with midazolam (2 mg) and fentanyl (50 mcg), followed by maintenance with dexmedetomidine. The procedure included crossing the aortic valve with a straight-tip guide supported by an AL 1.0 catheter and swapping with a Safari Extra Small wire. Aortic valvuloplasty was performed, followed by valve implantation. Postoperative imaging confirmed appropriate results. The patient remained stable throughout hospitalization and was discharged on SAPT with aspirin 100 mg daily. Echocardiographic evaluation of the bioprosthetic valve showed a Gmax/mean of 4/1 mmHg and DVI of 0.75. At the 45-day follow-up CT scan, there were no significant leaks or device-related thrombosis in either device. In conclusion, this case underscores the importance of tailored procedural and anesthesiologic planning to optimize transcatheter cardiovascular interventions outcomes in frail patients. Intracardiac ultrasound has a pivotal role for LAAO in patients with esophageal varices or high anesthesiologic risk.