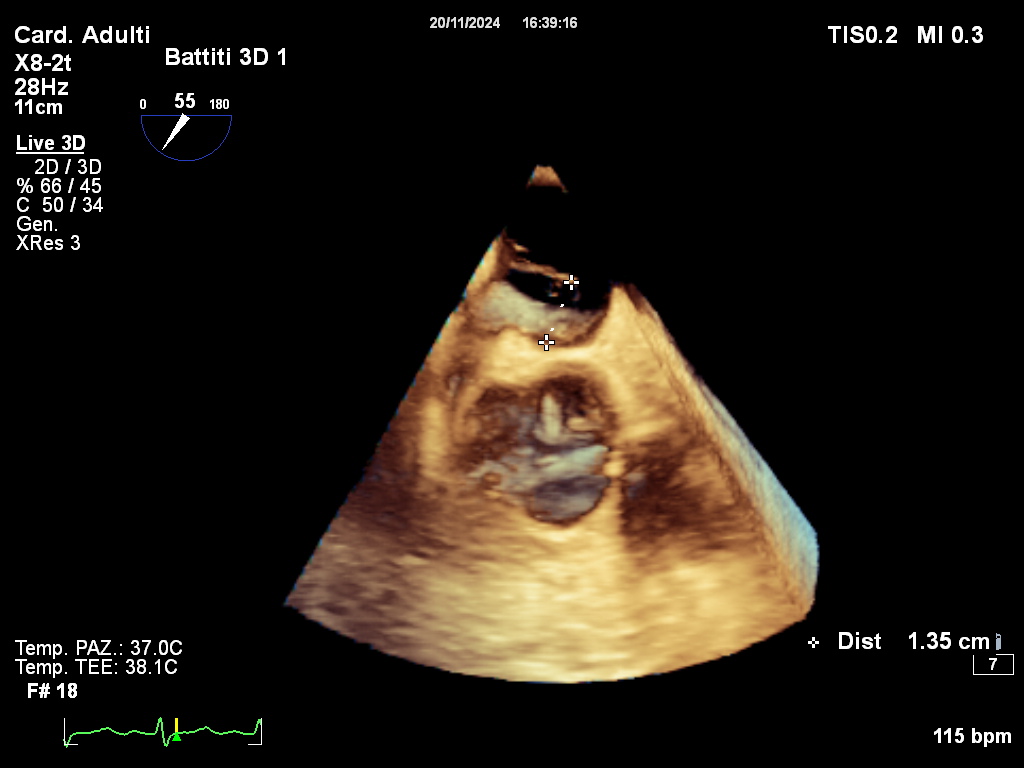
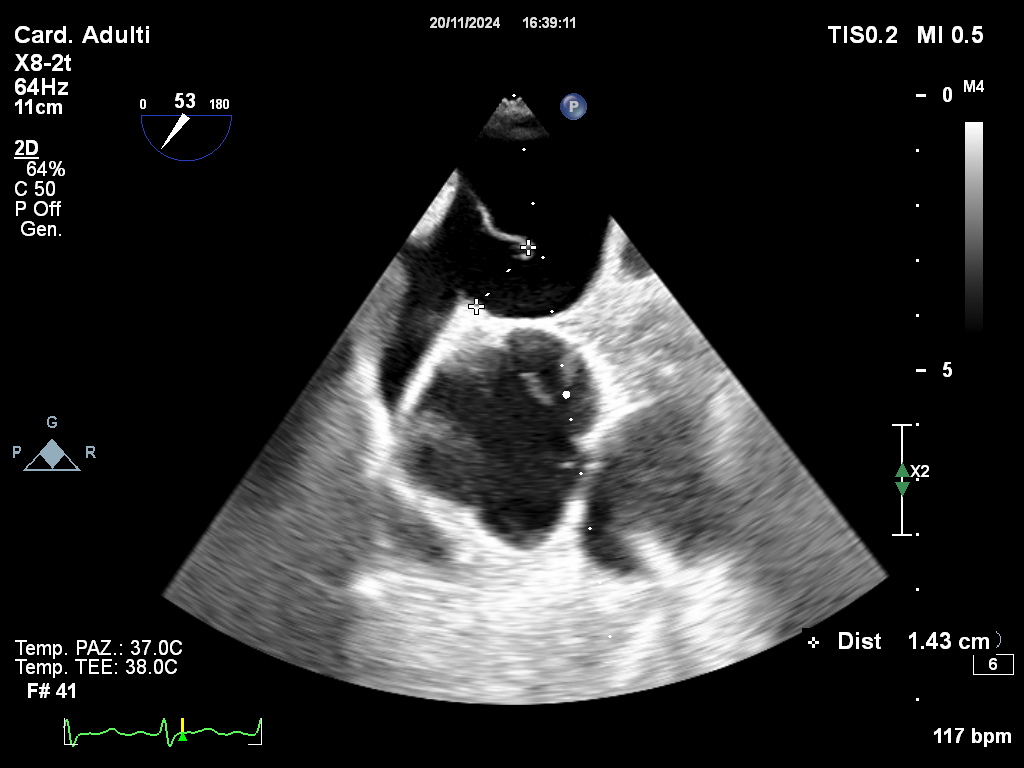
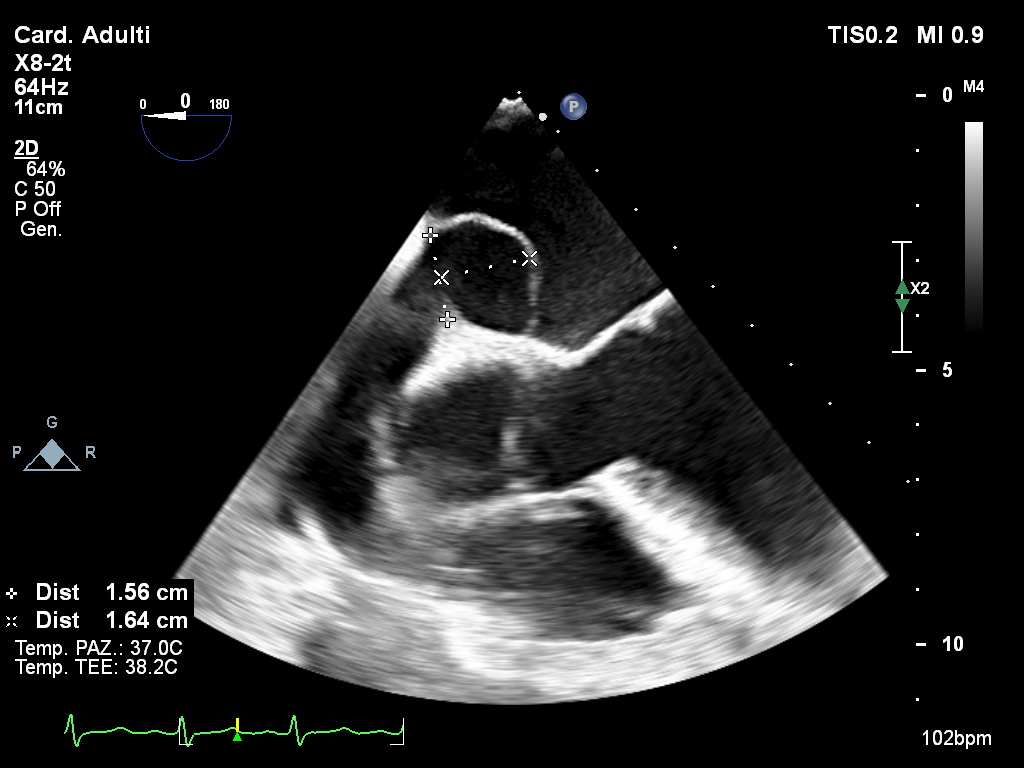
First described in the mid-20th century, platypnea-orthodeoxia syndrome (POS) is a rare condition characterized by positional shortness of breath and low blood oxygen levels. These features are triggered by standing and alleviated by clinostatism. It is most often linked to right-to-left shunting through a patent foramen ovale (PFO) or atrial septal defect, although its exact pathophysiology is not fully understood. Due to its rarity, POS is frequently underdiagnosed in many patients. The relationship between PFO and the occurrence of this condition may be influenced by aging-related factors such as aortic root dilation, PFO size, a projecting Eustachian valve (>10 mm), kyphoscoliosis (which distorts the interatrial septum), and right ventricular stiffness. Percutaneous closure of PFO in this subgroup of patients is recommended, even though approximately only 200 cases have been described since the first POS case was reported. It is crucial to perform a rigorous follow-up, especially in patients presenting these risk factors, which represent strong predictors of recurrence and short and long-term complications. We report a case of a 78-years-old woman that first illustrates the challenge of this diagnosis and second faces a therapeutic and follow-up approach. This patient presented with a history of previous multiple cryptogenic strokes, a recent myocardial infarction without any evidence of biventricular dysfunction. She presented refractory hypoxemia, showing several episodes of significant oxygen desaturation occurred she was in an upright position, but these were resolved upon repositioning to a recumbent posture, as confirmed by blood gas analysis. This raised suspicion of platypnea-orthodeoxia syndrome, reinforced by a positive transcranial doppler. A transesophageal echocardiogram (TEE) conducted with the patient lying flat revealed a hypermobile intra-atrial septum with a large PFO and right-to-left interatrial shunting necessitating closure of the defect. Our patient underwent a successful percutaneous closure of the communication (device 30-mm Gore Cardioform PFO occluder), with no residual shunting, clinical improvement, or positional hypoxemia. Starting from this case we will illustrate the challenge of understanding the exact mechanism by which POS results in clinical symptoms. We will also focus on the treatment possibilities according to the risk of recurrence, especially in subtypes of the population with certain anatomical risk factors.