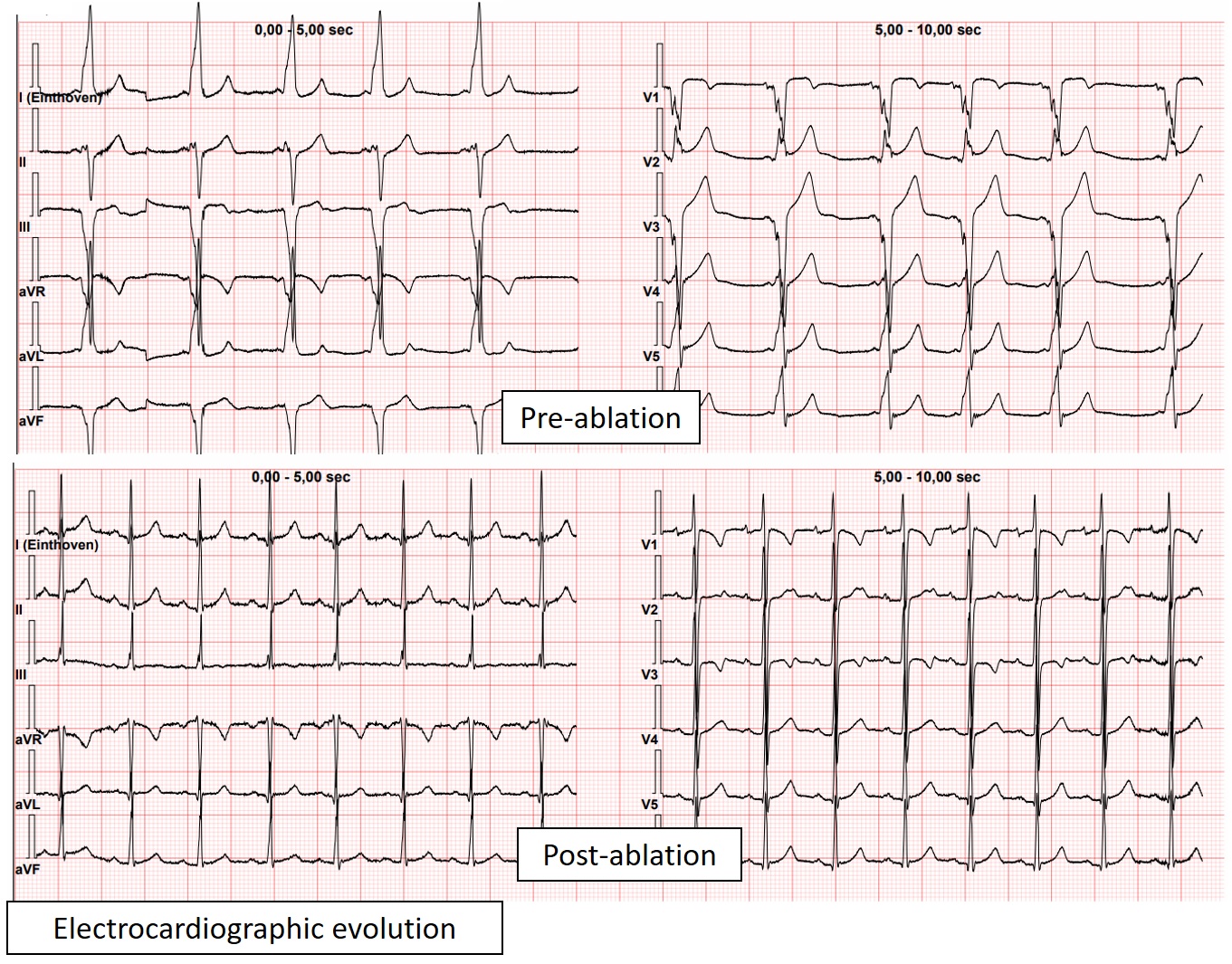
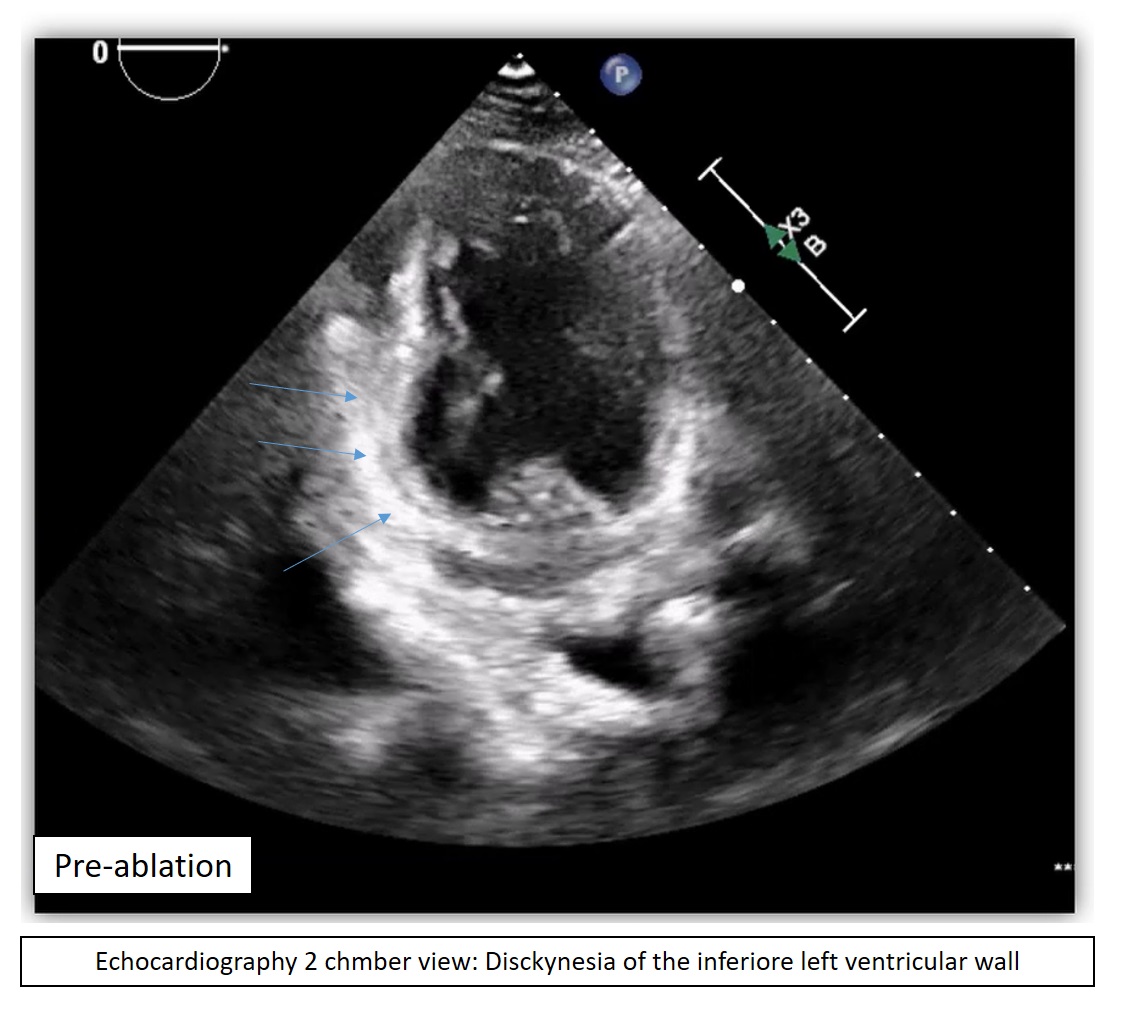
Introduction Considering ventricular pre-excitation exclusively as an electrical disorder may be reductive, as it overlooks the close relationship between electrical activation and mechanical cardiac function. Persistent ventricular pre-excitation may lead to left ventricular dyssynchrony, resulting in global or regional systolic dysfunction and justifying an interventional approach even in the absence of documented arrhythmias. We describe the case of a pre-adolescent patient who developed ventricular dysfunction secondary to ventricular pre-excitation. Case presentation A 12-year-old boy with a history of constant ventricular pre-excitation for approximately five years, without documented arrhythmias, had been treated for about one year with low-dose flecainide due to recurrent palpitations. Cardiological re-evaluation revealed left-sided ventricular pre-excitation on surface electrocardiogram. Transthoracic echocardiography showed a left ventricle of normal size, with mildly reduced global systolic function and dyskinesia of the inferior wall. Exercise stress testing demonstrated persistence of ventricular pre-excitation up to high heart rates (maximum heart rate 180 bpm), consistent with a high-risk accessory pathway. Based on the overall clinical picture, defined not only by electrocardiographic but also by echocardiographic findings, a multidisciplinary decision was made to proceed with an electrophysiological study and transcatheter ablation of the accessory pathway. Post-procedural evaluation demonstrated disappearance of ventricular pre-excitation on surface electrocardiogram, with repolarization abnormalities consistent with the electrical memory phenomenon. Echocardiography documented resolution of basal inferior wall dyskinesia and recovery of global systolic function. The patient was discharged in good general condition, without antiarrhythmic therapy. Conclusions This case highlights that persistent ventricular pre-excitation, even in the absence of documented arrhythmias, may lead to left ventricular dyssynchrony with subclinical systolic dysfunction, which is potentially reversible after catheter ablation. Persistence of anterograde conduction at high heart rates represents a key element in risk stratification, but should not be considered the sole criterion guiding the indication for electrophysiological study and ablative treatment in the pediatric population.