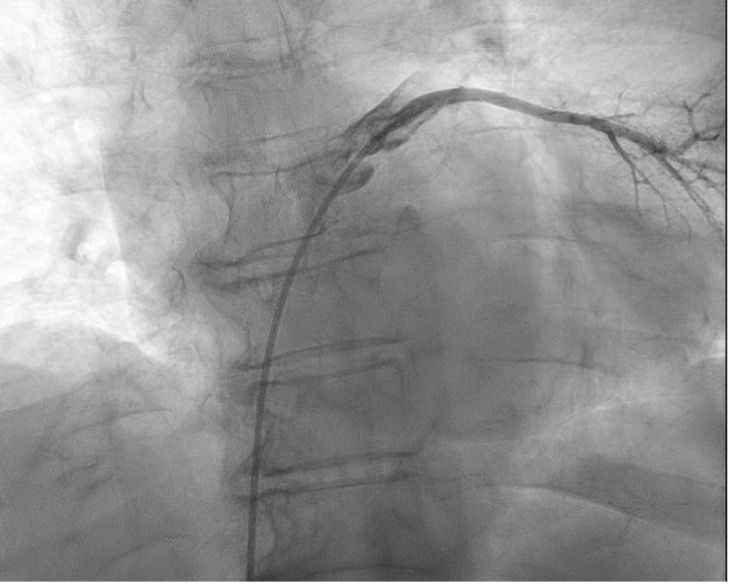
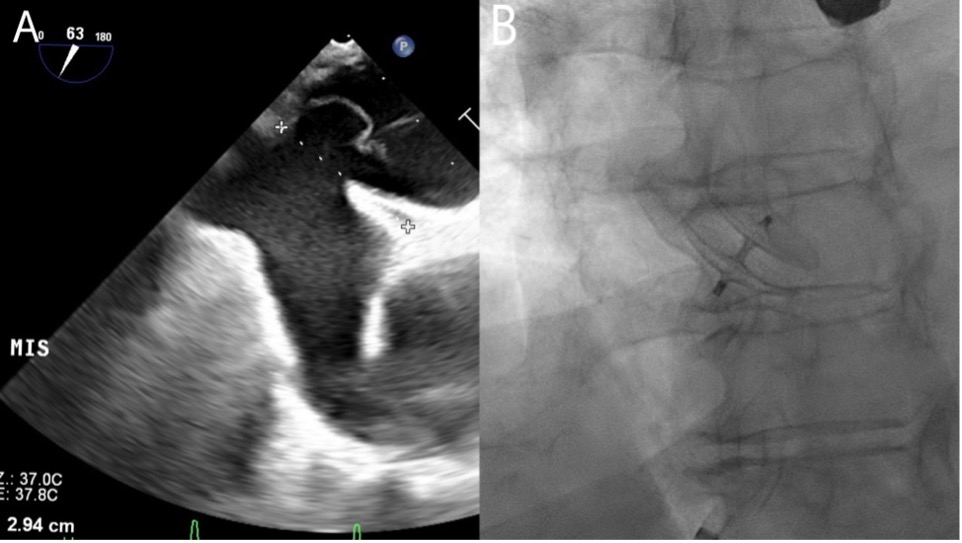
A 78 year old woman was admitted to emergency room for acute respiratory failure hypoxemic normocapnic. In past medical history: ischemic stroke; in the last month 3 episodes of absence in sitting position. In blood tests normal values of d–dimer and NT–proBNP; no evidence of lung disease on chest CT and no sign of pulmonary embolism. She was admitted to the Pneumology Department; during hospitalization the patient was found on her room chair disoriented and dyspneic; on blood gas analysis: p02 44 mmHg, pCO2 28 mmHg, P/F 44, SaO2 87%; on ECG sinus tachycardia. The patient was transferred in cardiac intensive care unit (CCU) where she was given high–flow oxygen therapy. In CCU a bedside chest x–ray was reported cranialization of the right hemidiaphragm. Seeing that dyspnea occurred only in upright position and never in supine position, a transthoracic echocardiogram with bubbles was performed witch showed right–to–left shunt. A transesophageal echocardiogram showed atrial septal aneurysm with patent foramen ovale (PFO) and a cardiac catheterization showed mild right–left shunt (Qp/Qs 0,81), with spontaneous passage of the catheter from the right atrium to the pulmonary vein through the patent foramen ovale during the procedure. After a multidisciplinary assessment, the patient was subjected to percutaneous closure of the foramen ovale with the placement of a device Amplatzer 25 mm, the patient was hospitalized for 10 days after the procedure and no further episodes of desaturation were observed. A 24–hour pulse oximetry showed no desaturation. At 2 months follow–up the patient no reported dyspnea and reports clinical well–being, confirming the diagnosis of platypnea–orthodeoxia syndrome (POS). Platypnea–orthodeoxia syndrome is characterized by episodes of paroxysmal dyspnea associated with desaturation that appear in the upright position and disappear in the supine position with no response to high flow oxygen. The cause of this syndrome is a shunt: extracardiac or often. Clinical manifestation of POS occurs when something stretches the site of shunt, in our case PFO, as a compression ab extrinsic (e.g. paralysis of the right hemidiaphragm). Multimodal imaging allow to find a cause of shunt. The therapy is the exclusion of the shunt with surgery or percutaneous intevention.