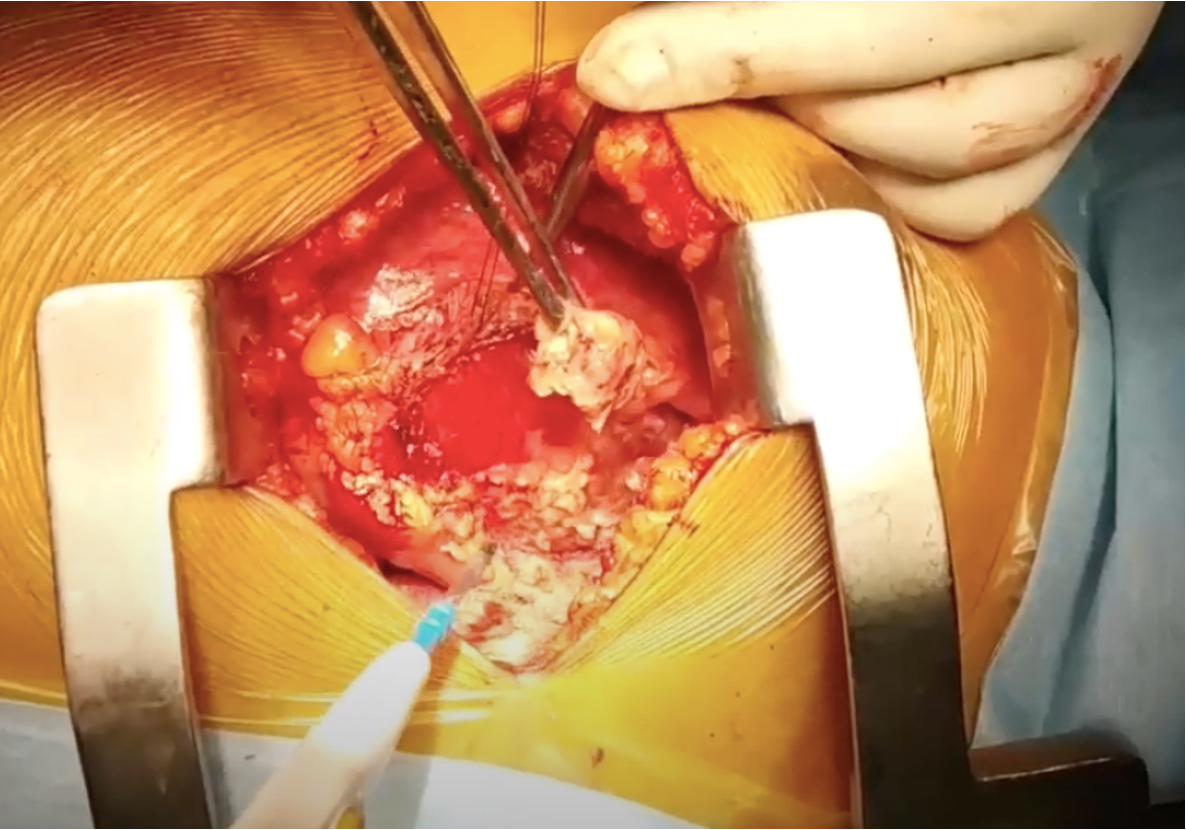
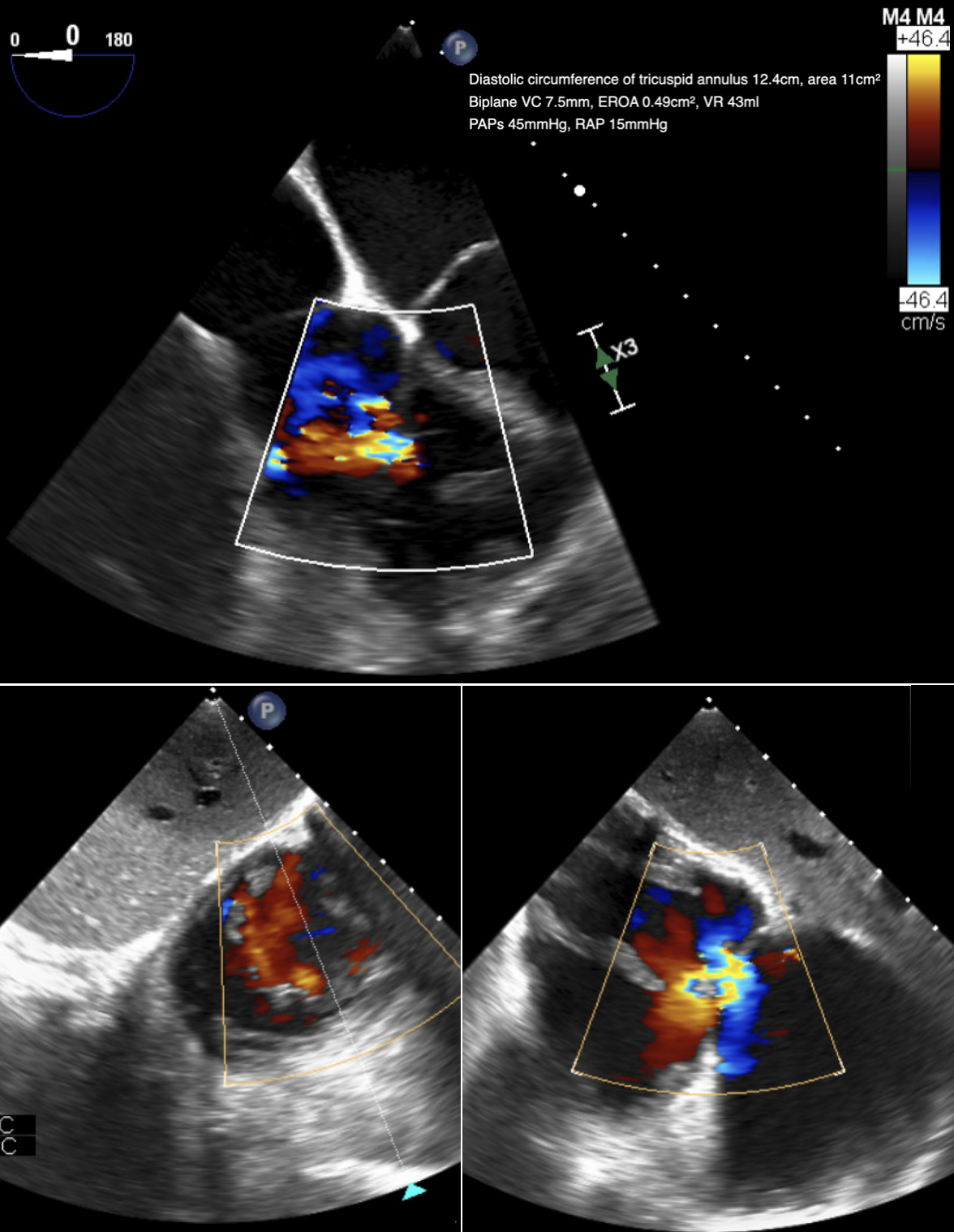
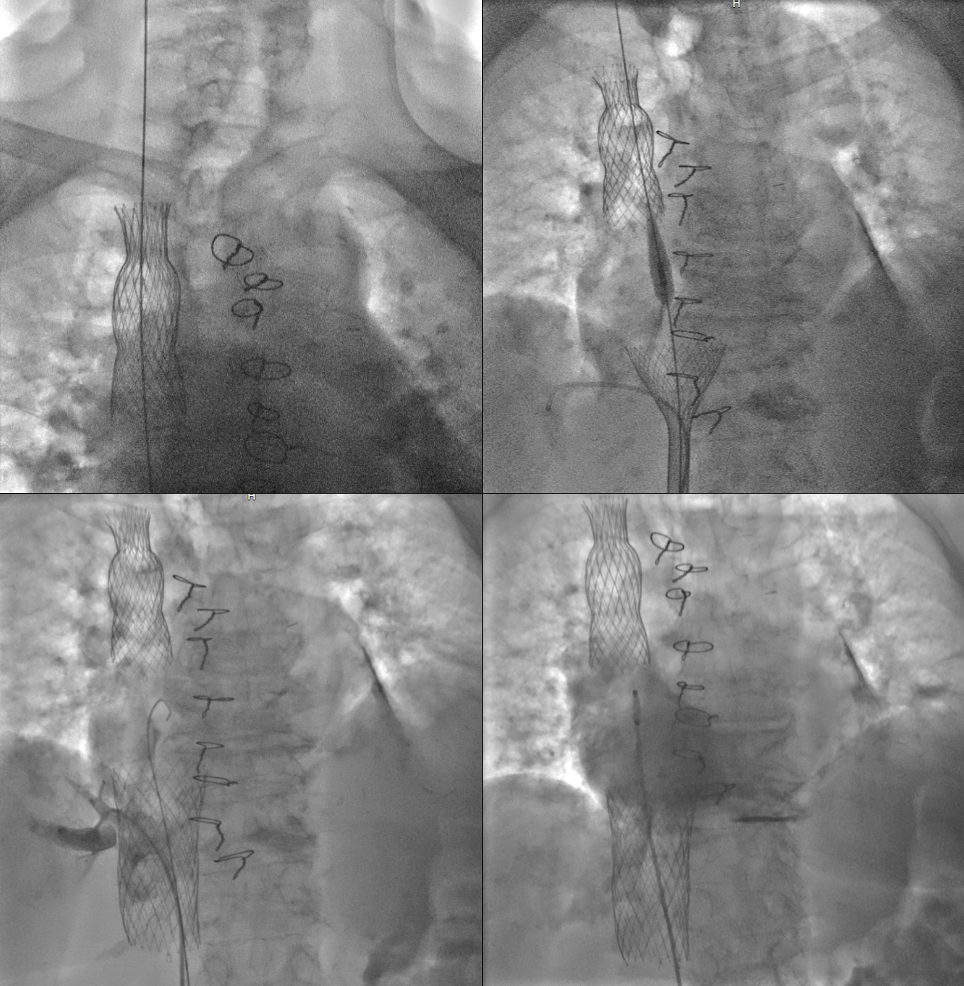
A 74-year-old woman presented with worsening dyspnea and leg swelling (NYHA IV) for one week. The patient had known arterial hypertension, diabetes mellitus II, AFib, moderate tricuspid insufficiency (TI), right HF requiring many hospitalizations, newly discovered radiation-induced constrictive pericarditis. Comorbidities included breast cancer treated with quadrantectomy and radiotherapy, restrictive respiratory deficit, chronic kidney disease, anemia, venous insufficiency, hepatitis, poliarthropathy. Chest x-rays and CT at presentation revealed pulmonary congestion, an enlarged cardiac silhouette, pericardial calcifications, hilar enlargement. After initial clinical improvement after medical therapy, TI was evaluated: given the multiple comorbidities, invasive procedures were not recommended. The recently diagnosed constrictive pericarditis was addressed by the Heart Team, confirming radiotherapy as causative agent: surgical pericardiectomy was performed. Thick calcified adhesions in the anterior and diaphragmatic pericardial surfaces were removed. The patient tolerated the procedure well and was discharged without complications (2021). Over the following 3 years, she underwent eight hospitalizations for worsening congestive symptoms and was managed pharmacologically. TI progressed to severe and pulmonary hypertension developed. During her latest hospitalization (08/2024), disabling symptoms had markedly worsened. High dose diuretics led to momentary clinical benefits. Tricuspid valvulopathy was re-evaluated. Transesophageal echocardiogram confirmed torrential TI. The right catheterization confirmed moderate pulmonary hypertension: RA 16mmHg, RV 16mmHg, PA 38mmHg, PCW 20mmHg. The case was discussed in Heart Team and the patient was referred for transcatheter bicaval valve system (TricValve) implantation. A 25mm TricValve was positioned in the SVC and a 35mm TricValve in the IVC. The procedure was performed with a transfemoral approach. Hepatic vein patency and reduced blood regurgitation from the atrium to the veins confirmed the successful result. At 4-month follow up, the patient reported complete functional recovery with significant symptoms improvement (NYHA II) and was free from HF rehospitalization. Echocardiographic signs corroborate the procedural success. This case confirms feasibility and safety of TricValve implantation for severe TI and reminds us of the importance of multidisciplinary evaluation in guiding therapy in complex patients.