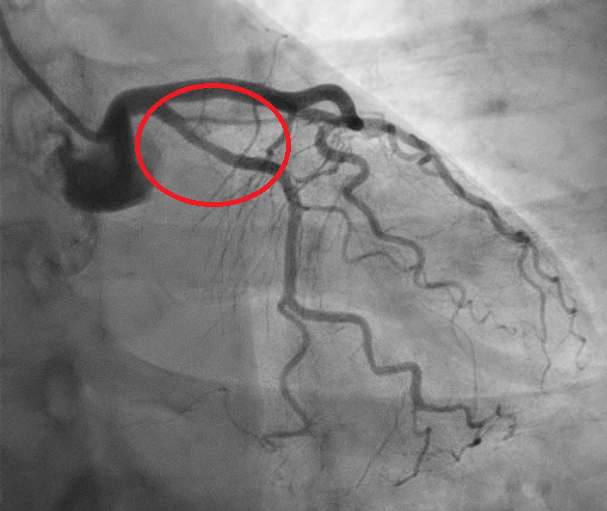
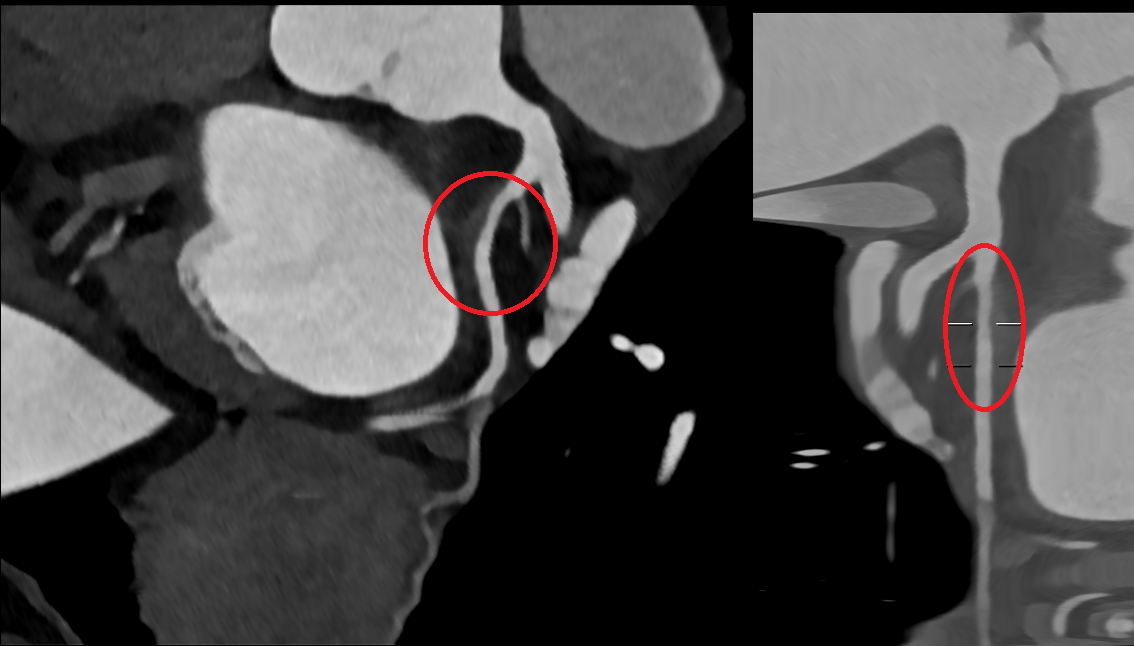
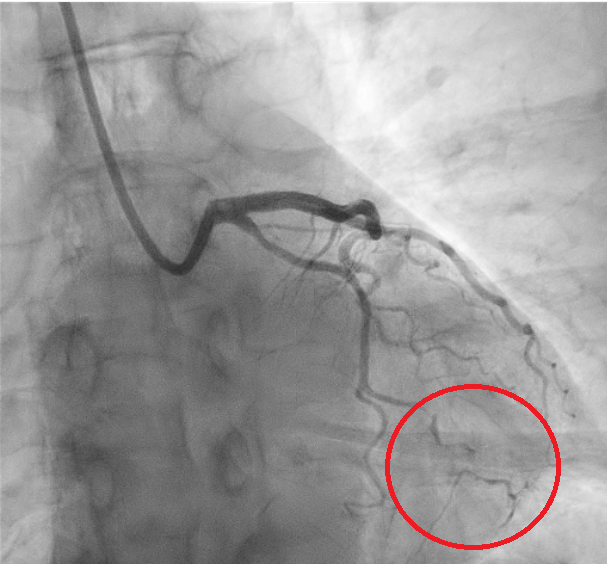
We report the case of a 61-year-old woman presenting with chest pain radiating to the left arm. EKG showed inferolateral repolarization abnormalities. Laboratory revealed mild elevation in troponin (0.76). Transthoracic echocardiography demonstrated mildly reduced systolic function with posterolateral wall akinesia (ejection fraction 48%). The patient was referred for coronary angiography showing no significant stenoses; however, a focal narrowing of the proximal circumflex artery (LCX) was observed, consistent with type 3 spontaneous coronary artery dissection (SCAD) according to the Yip–Saw classification (Fig. 1). Given the risk of iatrogenic propagation of the dissection and recommendations to minimize coronary instrumentation in SCAD, intracoronary imaging was avoided, and we performed instead coronary computed tomography angiography (CCTA) demonstrating mild stenosis of the LCX with mural hyperdensity, consistent with an intramural hematoma (Fig. 2). On day four, the patient experienced angina similar to the initial episode, with ECG changes and an increase in troponin (1.2). Repeat coronary angiography demonstrated progression of the dissection from the LCX to the distal segment of the first obtuse marginal branch, corresponding to evolution toward type IIb SCAD (Fig. 3). Given the limited myocardial territory at risk and the absence of ongoing symptoms, conservative management was continued. Patient was discharged on day ten on a beta-blocker and aspirin.with a planned follow-up CCTA at six months. This case highlights that in SCAD, particularly type 3 and proximal lesions, a conservative approach is often the safest strategy, with non-invasive imaging playing a key role in diagnosis, follow-up, and therapeutic guidance.