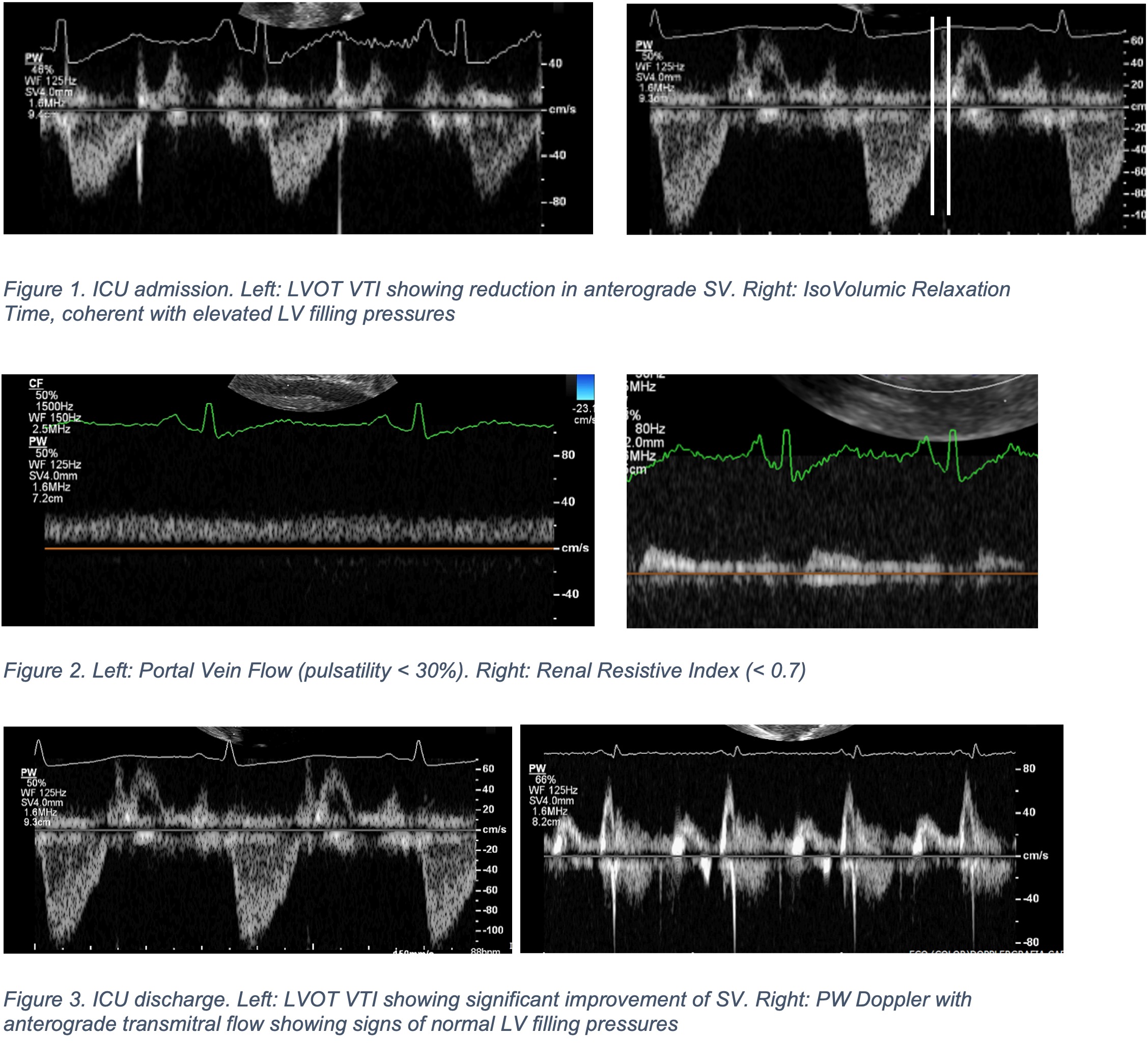
Introduction : Daily bed-side evaluation of echographic advanced parameters allows therapeutic tailoring in multiple scenarios. Case Presentation : A 63-year-old woman with no cardiac-related symptoms was admitted to the emergency department because of lower limbs paresthesias. The presence of significant peripheral hypereosinophilia and the results of the chest CT-scan were coherent with the suspect of eosinophilic pneumonia. The ECG showed diffuse ST-segment depression and hsTnI and NT-proBNP were elevated. The echocardiography revealed a diffusely-hypokinetic small-sized left ventricle ( LVOT VTI 10 cm, EF 35%), no signs of suboptimal ventriculo-arterial coupling (VAC 1.2), severe functional mitral regurgitation, elevation of left ventricular filling pressures (E/A 1, E wave 56 cm/s, IVRT 60 ms, Vp 40 cm/s) , normal indexes of right ventricular systolic function with signs of impaired relaxation (tricuspid E/A 1.2, E/e’ 5.5, presence of pre-systolic RVOT A-wave ), moderate tricuspid regurgitation with elevated pulmonary pressures (ePASP 40 mmHg), no splanchnic congestion (normal suvrahepatic vein flow, portal vein pulsatility index < 30%, renal vein stasis index 0) and no splanchnic hypoperfusion (renal resistive index 0.4). Endovenous diuretic therapy was started, without any vasodilator nor inotrope. A coronary CT-angiography ruled out obstructive CAD. The clinical suspect of eosinophilic myocarditis was raised and steroid therapy was started, without performing an invasive endomyocardial biopsy (EMB). The patient had an improvement in terms of anterograde cardiac output and filling pressures, with reduction of MR, TR and estimated pulmonary pressures; weight-adjusted low molecular weight heparin was also started because of left ventricular thrombus. A cardiac magnetic resonance was finally performed, with findings coherent with the hypothesis of eosinophilic myocarditis. Conclusion : in this case, two main aspects can be elucidated. The first insight is related to not performing an EMB, according to the 2024 ACC Expert Consensus on Myocarditis: the patient was classified as a stage B (asymptomatic) myocarditis, with an unfavourable estimated risk-benefit ratio. The second insight is related to the role of echodynamics in assessing the need for vasodilator, inotropic and diuretic therapy, especially in a scenario in which diastolic dysfunction plays a major role: daily evaluation allowed an accurate therapeutic optimization .