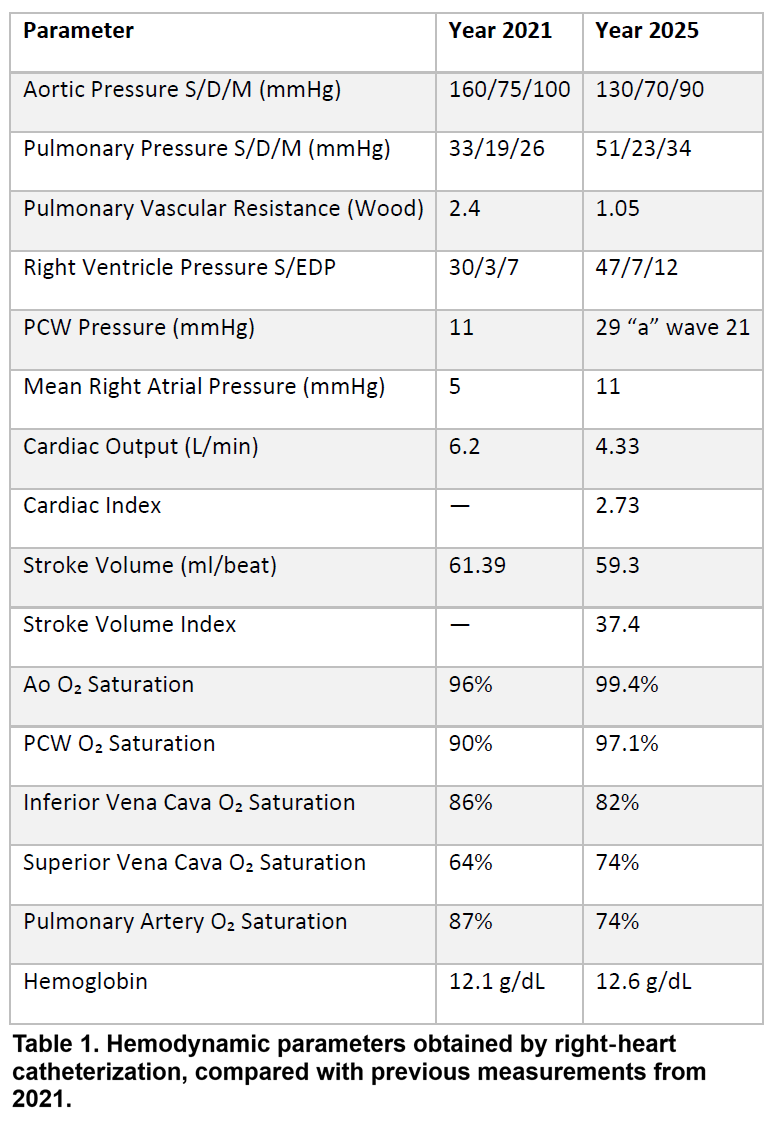
Background Pulmonary hypertension (PH) in systemic sclerosis (SSc) is a complex and heterogeneous condition, often classified as Group 1 pulmonary arterial hypertension (PAH). However, overlapping mechanisms—including left heart dysfunction (Group 2), interstitial lung disease (Group 3), and chronic thromboembolic disease (Group 4)—are frequent in patients with longstanding, multisystemic SSc. This overlap complicates therapeutic decisions, as pulmonary vasodilators, while beneficial in precapillary PH, may exacerbate heart failure in the presence of postcapillary involvement. This case highlights how dual vasodilator therapy can unmask a latent postcapillary component, leading to clinical decompensation, and supports the rationale for a more conservative, physiology-guided approach. Case Report A 75-year-old woman with longstanding SSc and multiorgan involvement was admitted for congestive heart failure. Her history included permanent atrial fibrillation, chronic respiratory failure, moderate chronic kidney disease, and diastolic dysfunction. She had been diagnosed with precapillary PH in 2021 (mPAP 26 mmHg, PVR 2.4 WU, PCWP 11 mmHg) and treated with bosentan, later switched to macitentan and tadalafil. At admission in November 2025, she presented with systemic congestion and worsening renal function. Echocardiography showed preserved systolic function, grade III diastolic dysfunction, and a chronic pericardial effusion. Right heart catheterization, performed while on dual therapy, revealed normalized PVR (1.05 WU) but a significant rise in PCWP (29 mmHg), indicating a shift toward postcapillary PH (table 1). Intravenous hydration improved renal function and reduced pericardial effusion. Given the hemodynamic profile and clinical response, tadalafil was discontinued, while macitentan and diuretics were maintained. The patient was discharged in stable condition with close follow-up. Conclusions This case underscores the potential harm of overtreatment in SSc-associated PH. While dual vasodilator therapy is standard in PAH, it may unmask or worsen a postcapillary component in patients with mixed or evolving hemodynamics. In such cases, monotherapy with an ERA may offer a safer and more effective strategy. Careful hemodynamic monitoring and individualized treatment are essential to avoid iatrogenic decompensation. In SSc-PH, treating less may sometimes mean treating smarter.