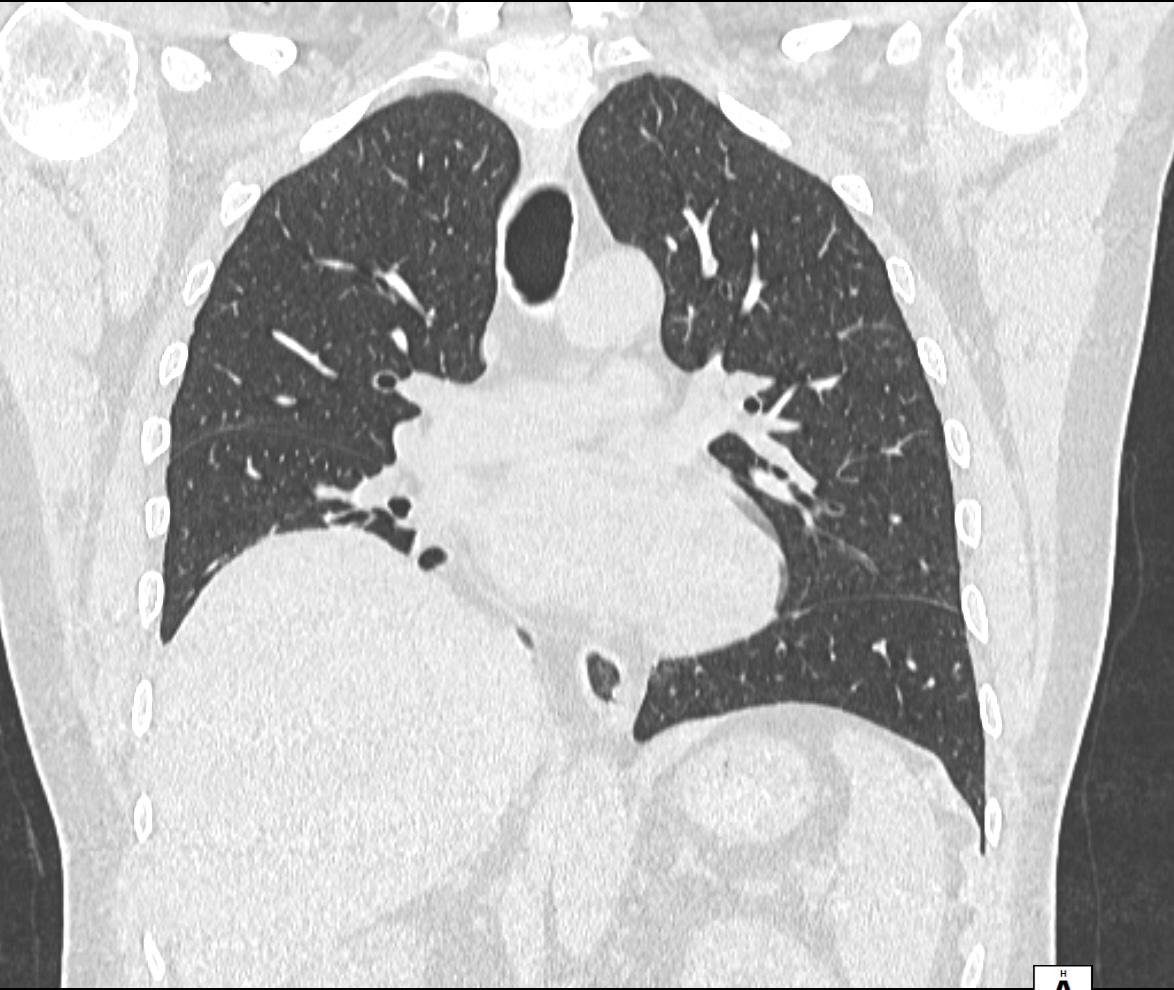
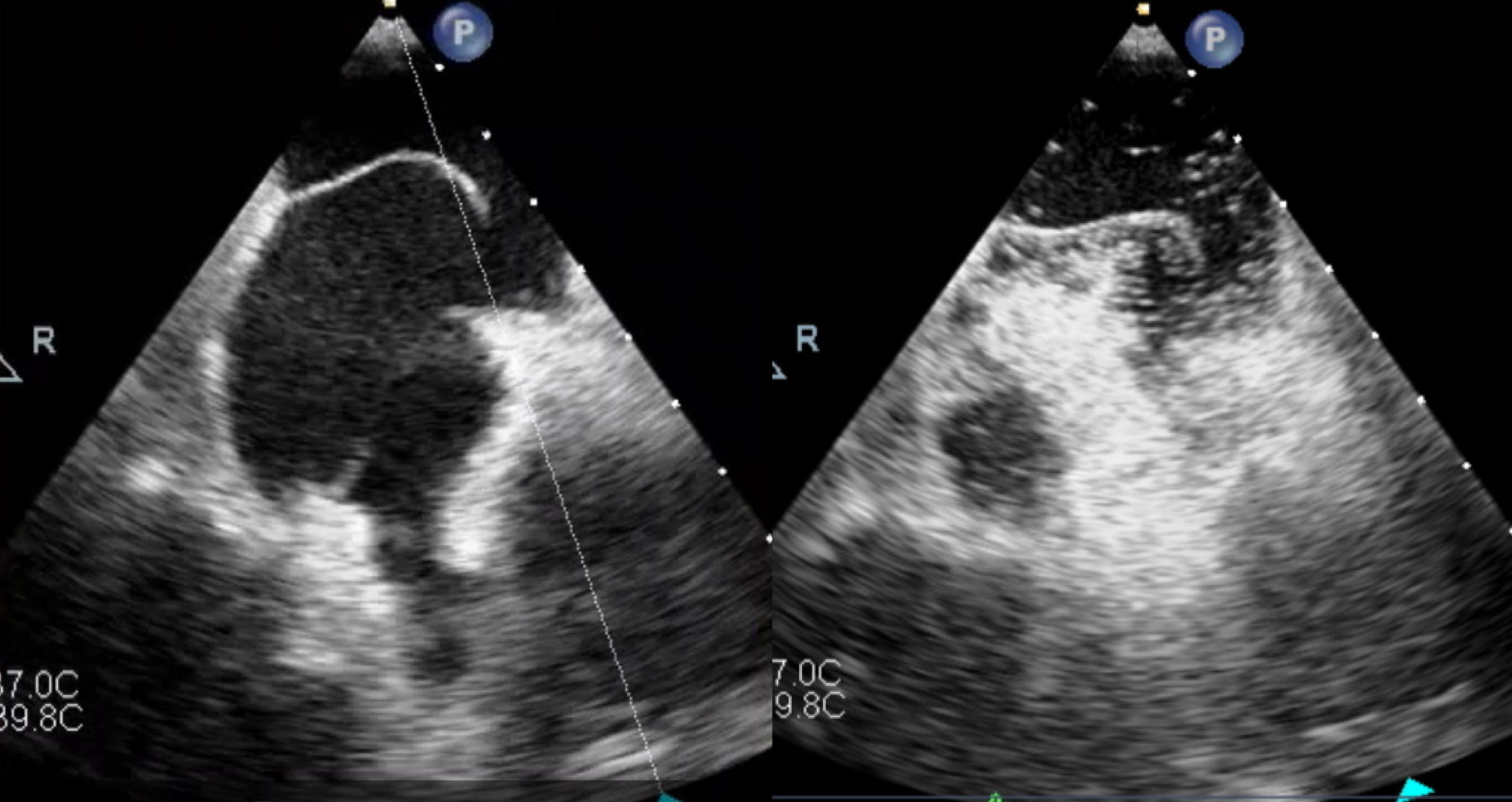
Platypnea-orthodeoxia syndrome (POS) is a rare condition characterized by dyspnea and arterial desaturation in the upright position (orthodeoxia), which resolve or improve in the supine position (platypnea). The pathophysiological mechanism requires two components: an anatomical substrate for a right-to-left shunt, either cardiac—most commonly a patent foramen ovale—or extracardiac, such as pulmonary arteriovenous malformations, together with a functional or dynamic factor that enhances shunt flow in the upright position, including changes in intrathoracic pressure or cardiac geometry. We report the case of a 62-year-old man with no prior cardiovascular history who presented to the emergency department with severe hypoxemia (SpO₂ 74%) despite being eupneic at rest, and with markedly elevated D-dimer levels. One week earlier, he had been hospitalized for acute perforated cholecystitis and had undergone emergency laparoscopic cholecystectomy, followed by discharge after a short, uneventful postoperative course. On clinical evaluation, the patient was asymptomatic despite marked hypoxemia. Arterial blood gas analysis confirmed hypoxemic respiratory failure with a significant postural variation: PaO₂ was 52 mmHg in the supine position and decreased to 37 mmHg when upright, while PaCO₂ and lactate levels remained within normal range. Given the recent surgery and elevated D-dimer levels, pulmonary embolism was initially suspected. Contrast-enhanced chest CT revealed a subsegmental pulmonary embolism in the left lower lobe, a small peribronchial consolidation, and marked elevation of the right hemidiaphragm, which had not been present on preoperative imaging (figure 1) However, the limited thromboembolic burden did not adequately explain the severity and positional nature of hypoxemia, raising suspicion of platypnea–orthodeoxia syndrome. Transthoracic echocardiography with contrast suggested a patent foramen ovale (PFO), which was subsequently confirmed by transesophageal echocardiography with bubble study, demonstrating a significant right-to-left shunting (Figure 2) The patient underwent PFO closure, resulting in a marked improvement in arterial oxygenation in both the supine and upright positions. POS is a rare but reversible cause of positional hypoxemia. Clinical suspicion is key to timely diagnosis. Correction of the underlying anatomical substrate can lead to rapid and sustained improvement in arterial oxygenation and patient outcomes.