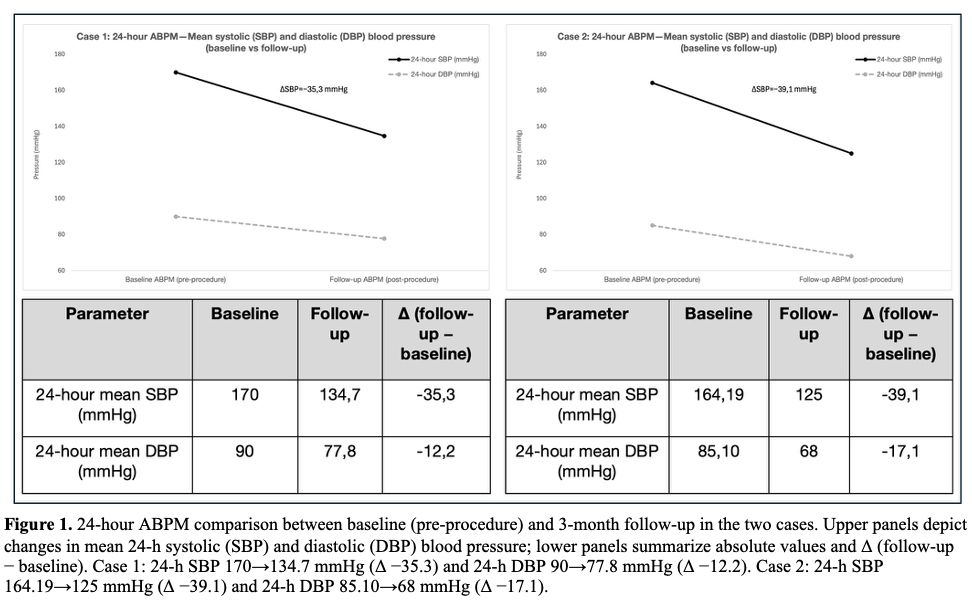
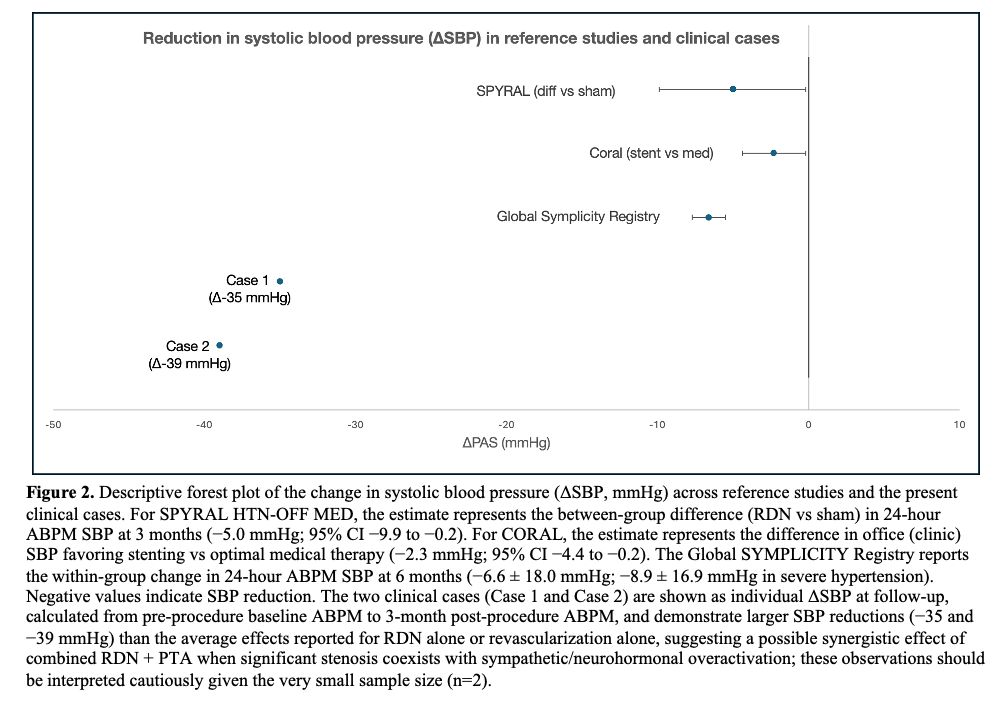
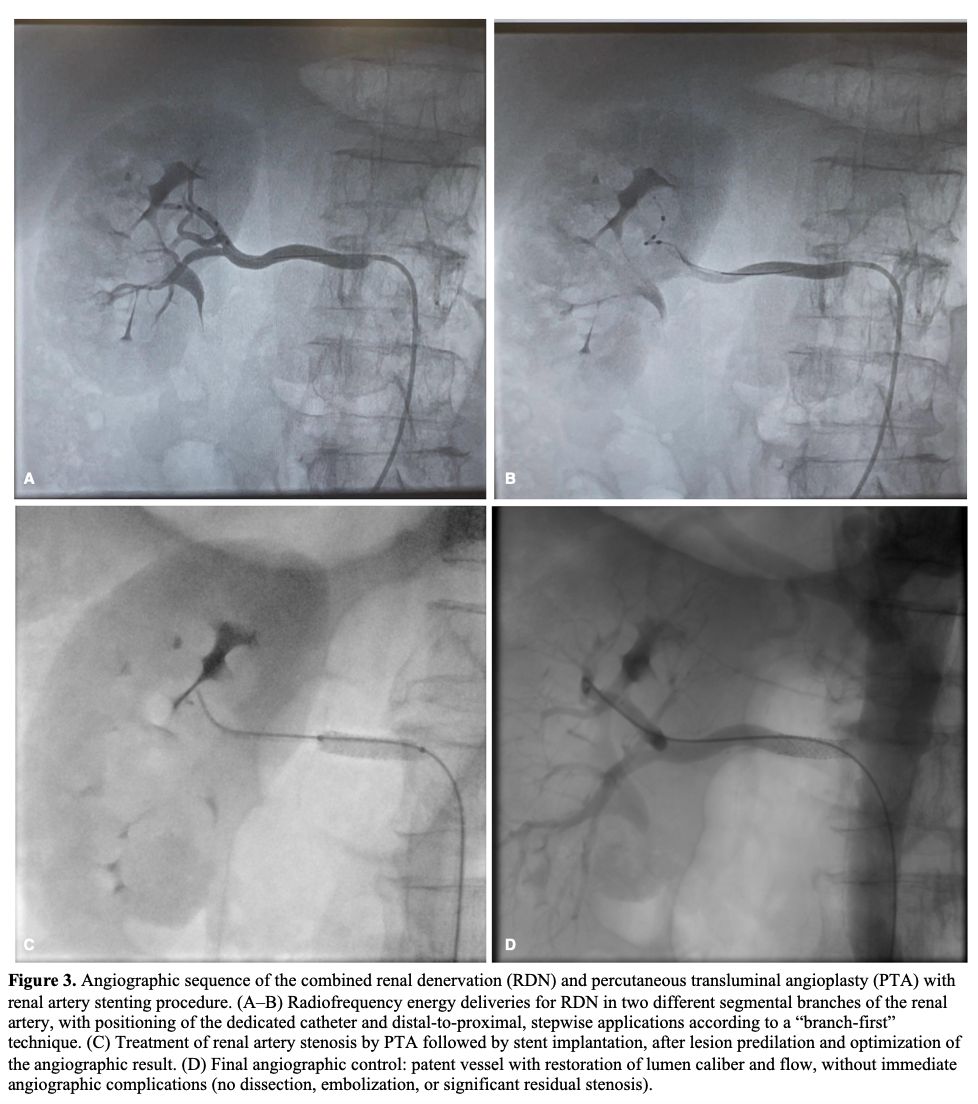
BACKGROUND. In resistant renovascular hypertension, blood pressure (BP) reduction after renal revascularization may be less than expected, suggesting that restoration of renal blood flow is not always sufficient to switch off the neurohormonal and sympathetic activation induced by renal artery stenosis. Catheter-based renal denervation (RDN), by modulating renal and systemic sympathetic overactivity, may complement the effect of percutaneous transluminal angioplasty (PTA) with possible stent implantation. CASE SERIES. We report two patients managed within the FEDERICUS registry pathway who underwent a combined strategy of radiofrequency (RF) RDN plus renal PTA/stenting. Case 1 (54-year-old man) with resistant hypertension on multi-drug therapy underwent RF-RDN (complete on the left and mid-to-distal on the right) and, during the same session, right renal PTA with implantation of two overlapping drug-eluting stents, achieving a good final angiographic result. Case 2 (75-year-old man) with severe renovascular disease: angiography showed a severe (90%) para-ostial stenosis of the right renal artery with chronic left ostial occlusion; mid-to-distal RDN was performed followed by implantation of a covered stent on the right, with an uneventful course.At 3-month follow-up, ABPM showed a clinically relevant reduction expressed as Δ (follow-up − baseline): Case 1: Δ24-h SBP/DBP −35.3/−12.2 mmHg; Case 2: Δ24-h SBP/DBP −39.1/−17.1 mmHg. In both cases, treatment de-escalation was observed compared with the pre-admission home regimen: discontinuation of doxazosin in Case 1; discontinuation of nifedipine and dapagliflozin in Case 2 CONCLUSIONS. Available evidence indicates that RDN produces a moderate BP reduction, more evident for SBP and on ABPM: in SPYRAL HTN-OFF MED, the between-group difference (RDN vs sham) for the change in 24-h SBP at 3 months was −5.0 mmHg (95% CI −9.9 to −0.2), consistent with an approximately 5 mmHg short-term reduction; in CORAL, the SBP difference favoring stenting was −2.3 mmHg (95% CI −4.4 to −0.2; p=0.03). In our two cases, the combined RDN + PTA approach was associated with a larger SBP reduction than that reported on average in studies evaluating RDN alone or revascularization alone, supporting the hypothesis that PTA and RDN may be synergistic rather than alternative when significant stenosis coexists with neurohormonal/sympathetic overactivation. This observation should be interpreted with caution given the limited sample size (n=2)