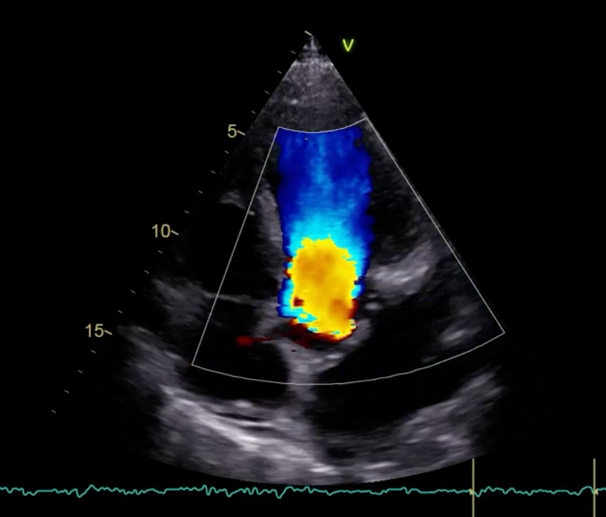
Case Presentation: A 54-year-old man presented with acute chest pain, rapidly worsening dyspnea, and intermittent fever over two months. ECG showed junctional ectopic tachycardia and incomplete left bundle branch block. Blood tests revealed elevated Hs-TnI (616-2993 pg/ml) and NT-proBNP (14,970 pg/ml). Medical history included eosinophilic granulomatosis with polyangiitis (EGPA), moderate-to-severe aortic regurgitation, and hypertension. Investigations and Management: Transthoracic echocardiography revealed severe aortic regurgitation, left ventricular dysfunction (EF 40–45%), pericardial effusion, and a floating aortic valve image suggestive of an intimal flap. CT angiography excluded aortic dissection but confirmed incomplete aortic cusp coaptation. Despite oxygen therapy, NIV, and aggressive diuresitic therapy, the patient deteriorated, developing cardiac arrest with pulseless electrical activity (PEA). ROSC was achieved after advanced life support (ALS). Transesophageal echocardiography showed torrential aortic regurgitation, necessitating emergency valve replacement. Intraoperatively, the ascending aorta exhibited a dense fibrinoid layer, and the valve showed retracted cusps. Histopathology confirmed EGPA-related vasculitic involvement with fibrinoid necrosis, eosinophilic infiltrates, and angioplasia. Outcome: The post-operative course was uneventful apart from transient atrial fibrillation. The patient was discharged on intensified immunosuppressive therapy, including mycophenolate and increased mepolizumab. At three-month follow-up, echocardiography showed stable findings and an EF of 54%. Discussion: Cardiac involvement in EGPA, though rare, significantly impacts prognosis and is more common in ANCA-negative patients. This case is unique due to angioplasia and vasculitis on histopathology, features not previously described in EGPA-related aortic regurgitation. Early recognition and aggressive management are critical. CMRI remains the gold standard for detecting cardiac involvement in EGPA, emphasizing the importance of periodic evaluation. Conclusion: This case highlights the life-threatening potential of EGPA-related cardiac complications, underscoring the need for heightened awareness and interdisciplinary management to improve outcomes in these often young patients.