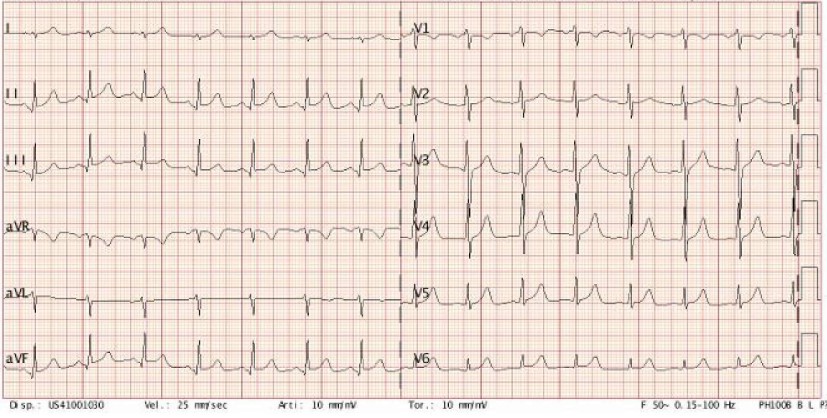
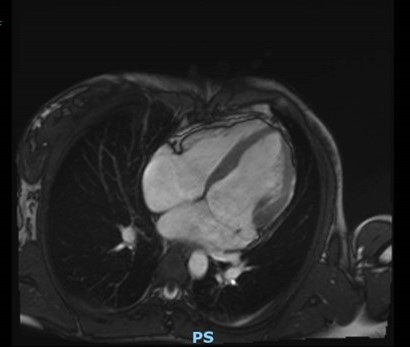
Introduction: Mitral annular disjunction (MAD), often associated with mitral valve prolapse (MVP), is a structural heart abnormality that predisposes to severe arrhythmias and sudden cardiac death (SCD), particularly in young patients. We present the case of an 18-year-old woman with MVP and MAD who survived an out-of-hospital cardiac arrest (OHCA), highlighting diagnostic challenges and therapeutic strategies. Case Presentation: An 18-year-old woman, with a history of mild mitral regurgitation (MR) in the context of MVP, experienced OHCA due to ventricular fibrillation. She was resuscitated and admitted to the Cardiac Intensive Care Unit of San Paolo Hospital (Savona). Echocardiography at admission revealed moderate MR with bileaflet MVP, a 16-mm MAD, and moderate biventricular dysfunction. Post-resuscitation ECGs showed sinus rhythm with nonspecific repolarization abnormalities. Blood tests ruled out hormonal or electrolyte imbalances. In-hospital rhythm monitoring revealed brief episodes of monomorphic non-sustained ventricular tachycardia, resolved after starting beta-blocker (BB) therapy. Cardiac MRI further confirmed MAD, moderate MR with bileaflet MVP, quantifying a left ventricular ejection fraction (LVEF) of 37% and a right ventricular (RV) ejection fraction of 40%, without LGE. Differential diagnoses included arrhythmic MVP syndrome and primary cardiomyopathy with MR as a bystander. Genetic testing for cardiomyopathy-related mutations was performed to investigate this hypothesis, but results are pending. The patient was discharged after the implantation of a subcutaneous ICD and the initiation of anti-remodeling therapy with ACE inhibitor and MRA, along with BB. Follow-up at 1 and 3 months showed clinical stability (NYHA class I), and no arrhythmic events. Coronary CT excluded significant stenoses or anomalous coronary origins. Serial echocardiograms showed recovery of RV function and partial improvement of LVEF up to 45%, with persistent moderate organic MR. On the therapeutic side, ACE inhibitor was titrated, but the patient declined SGLT2 inhibitor. Conclusions: This case highlights the role of MAD as a potential substrate for life-threatening arrhythmias in MVP. Advanced imaging is crucial for confirming the diagnosis and evaluating high-risk features of SCD. Imaging and genetic testing also help identify an underlying cardiomyopathy. Long-term follow-up is essential to monitor MR progression and assess the need for cardiac surgery.