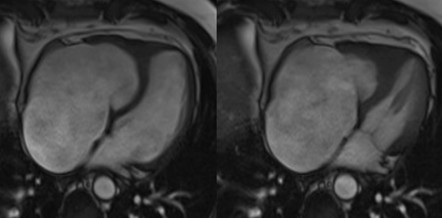
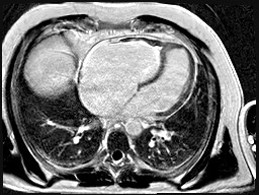
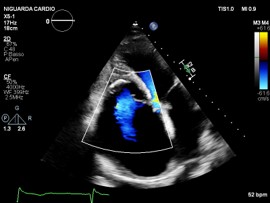
We report the case of a 48-year-old male with chronic eosinophilic leukaemia (CEL) complicated by multiorgan damage, including chronic kidney disease (CKD) and liver disease with recurrent ascites. Cardiac follow-up began at CEL diagnosis. The patient remained stable until 2015, when he underwent two atrial tachycardia ablations. Cardiac magnetic resonance imaging suggested Loeffler endocarditis, showing right ventricle (RV) fibrosis, mildly impaired RV systolic function and severe tricuspid regurgitation (TR). The left ventricle (LV) remained preserved. Cardiac computed tomography excluded coronary disease. In June 2025, despite guideline-directed medical therapy, the patient developed severe dyspnea, massive ascites and acute kidney injury on CKD. Transthoracic (TTE) and transoesophageal echocardiography showed torrential TR not amenable to percutaneous repair. Laboratory results showed normal blood count, serum creatinine 5.5 mg/dL, bilirubin 2 mg/dL, NT-proBNP 7950 pg/mL. Electrocardiography showed junctional rhythm. On admission, intravenous furosemide was continued. A 5-L paracentesis yielded negative cytology and microbiology. TTE confirmed severely dilated RV and atrium, paradoxical septal motion, hypokinetic RV and torrential TR. LV function was normal. Right heart catheterization revealed reduced cardiac index (2.04 L/min/m²), mildly elevated pulmonary capillary wedge pressure (14 mmHg), normal pulmonary pressures (24/15/19 mmHg), normal pulmonary vascular resistance (1.3 WU) and elevated right atrial pressure (19 mmHg). Low dose dopamine (2 mcg/kg/min) improved perfusion and diuresis, leading to clinical stabilization with weight loss (−19 kg), waist reduction (−11 cm), and improved labs. Multisystem evaluation was undertaken. Portal hypertension and decompensated liver disease were excluded. Liver biopsy revealed extensive fibrosis without cirrhosis or malignancy. MELD-XI was 48. Haematology confirmed longstanding CEL remission. Imatinib was discontinued, with monthly molecular monitoring. Renal function normalized under inotropes, with no further tests needed. Extracardiac and serologic workup was negative. Blood type: B Rh+. The case was reviewed by the transplant team. No absolute contraindications to heart transplantation were found. Combined heart–liver transplantation was deemed unnecessary given the absence of cirrhosis. LVAD was excluded. On August 1st, 2025, the patient was listed for urgent heart transplantation (Urgency level 2).