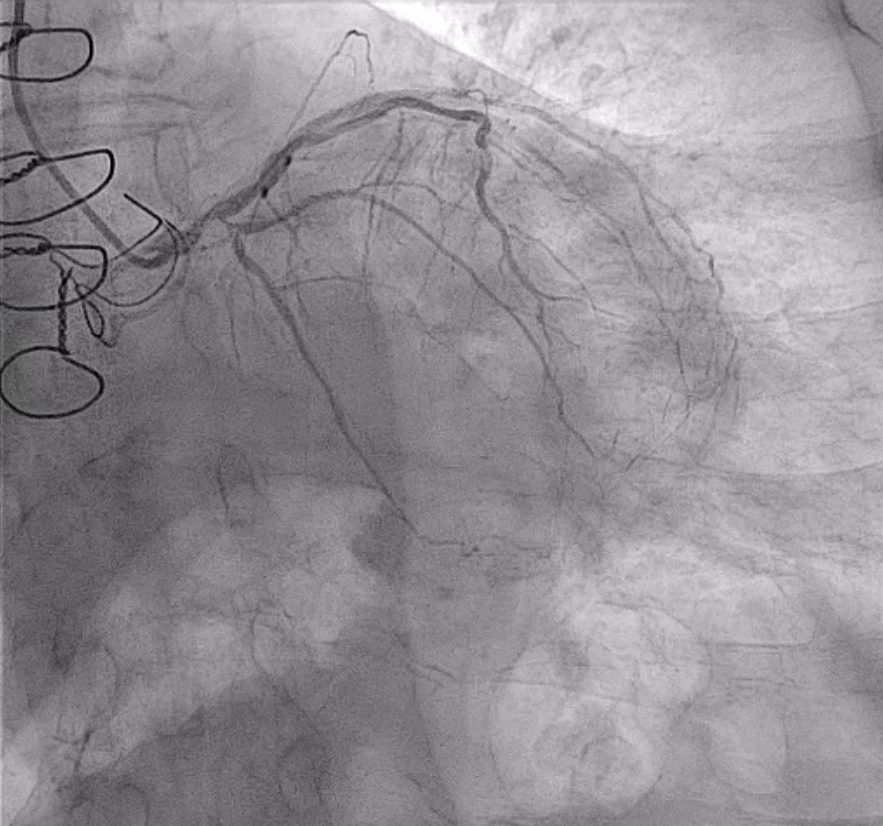
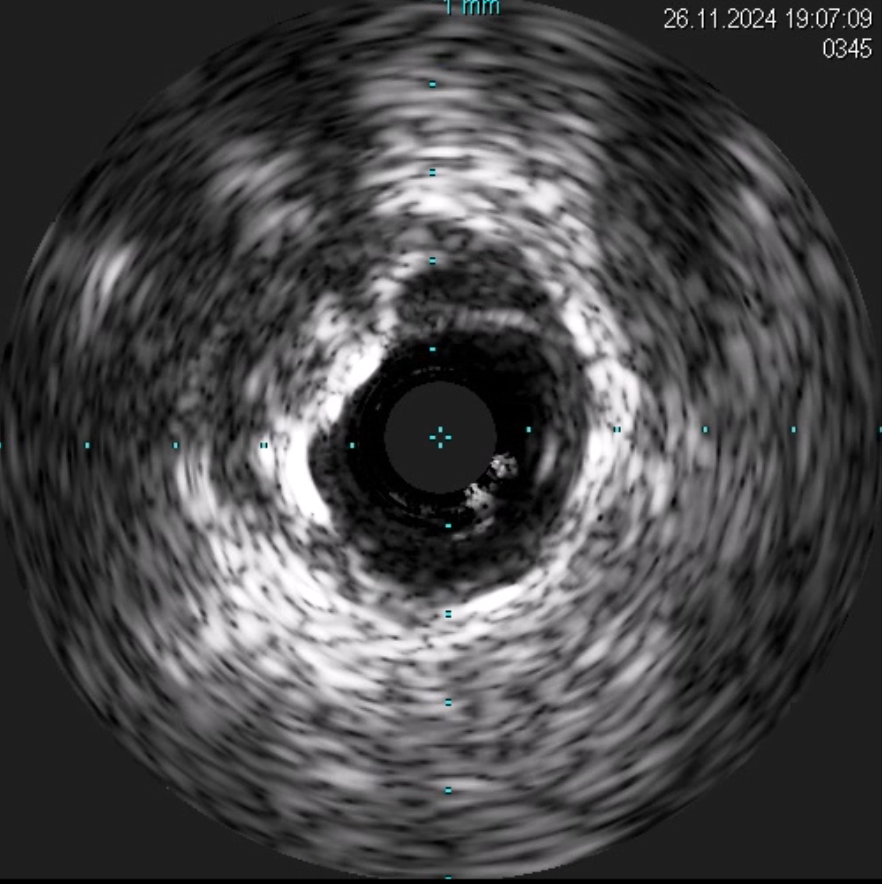
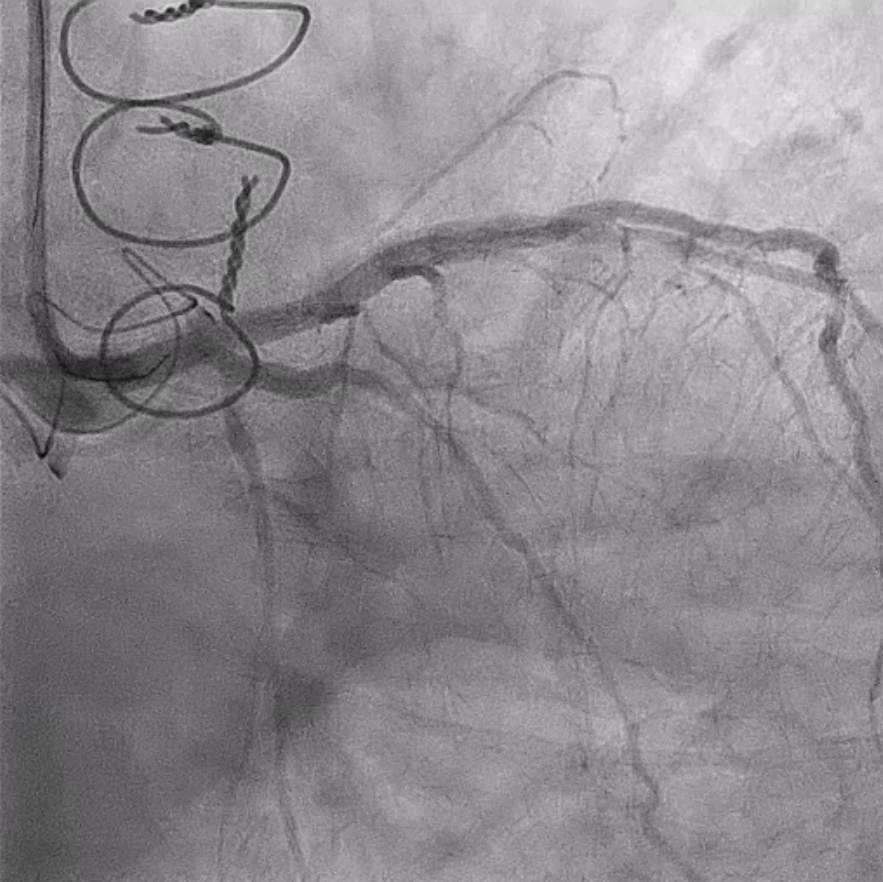
An 80-year-old male patient was admitted for symptomatic congestive heart failure, presenting with progressive dyspnea (NYHA class III). He has type 2 diabetes and moderate chronic kidney disease, and his cardiological history includes post-infarction dilated cardiomyopathy, permanent atrial fibrillation, and a surgical aortic valve replacement with a bio-prosthesis. An ECG showed previous inferior necrosis, and high-sensitivity cardiac troponins were elevated and indicative of acute myocardial damage. The echocardiogram revealed hypokinetic-dilated cardiomyopathy with severe systolic dysfunction (EF 30%), good function of the aortic prosthesis, moderate to severe regurgitation of the atrioventricular valves, and pulmonary hypertension. Coronary angiography demonstrated severe three-vessel disease involving the left main coronary artery, characterized by an extensive calcific burden. Following a Heart Team discussion, the patient was deemed unsuitable for surgery due to extremely high operative risk, given the number, extent, and complexity of the calcified lesions. Therefore, the patient was considered for percutaneous revascularization of the left coronary artery via right radial access. Considering the anatomical challenges, PCI was performed under IVUS guidance. Lesion preparation included the use of a microcatheter to facilitate guidewire advancement, followed by initial debulking with non-compliant balloons and intravascular lithotripsy using Shockwave technology. Drug-eluting stents were subsequently implanted from the left main coronary artery to the left anterior descending and left circumflex branches using the TAP technique. Final optimization was achieved with kissing balloon inflation and the proximal optimization technique (POT). Advanced techniques, including intravascular imaging, microcatheters, and intravascular lithotripsy, are essential for managing calcified left main coronary lesions, ensuring precise lesion preparation and stent expansion. These methods improve procedural success and long-term outcomes, especially in patients with complex coronary anatomies.