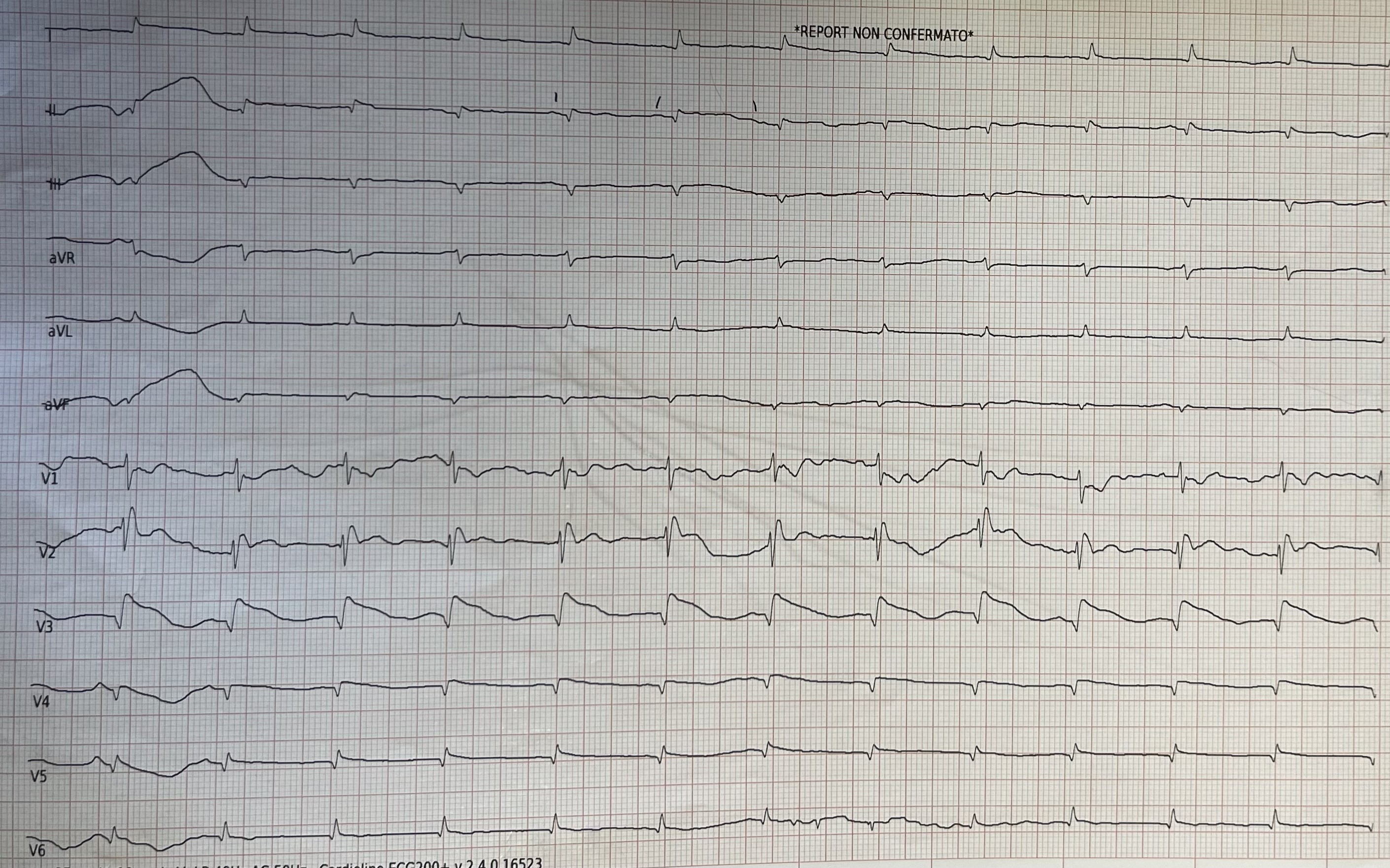
A 75 years old female patient was admitted to our Coronary Care Unit for suspected acute coronary syndrome during sepsis likely originating from an endovascular device, with history of recent syncopal episodes. Coronary angiography ruled out significant coronary artery disease. An ECG perfomed during hospitalization revealed a Brugada Syndrome (BrS) type 1 pattern (coved ST-segment elevation in leads V1-V3), not previously present. Blood tests showed leukocytosis and elevated CRP. The patient’s hemodynamic condition required vasopressor support, consistent with septic shock. Several studies have explored the link between inflammation and septic status with BrS. Endothelial, metabolic, and immune response abnormalities play a key role in the pathogenesis of arrhythmias during sepsis. Impaired autoregulation of blood flow in the coronary microcirculation and altered metabolism contribute to these issues. Septic myocytes often switch their primary energy source from free fatty acids to glucose, negatively impacting contractility, similar to the effects seen in post-ischemic myocardial hibernation¹. Pathogen-associated molecular patterns and damage-associated molecular patterns, released by pathogens or damaged tissues, activate pro-inflammatory cytokines patwhays (TNF-α, IL-1β, IL-6, C5a) that lead to mitochondrial dysfunction, disrupt calcium homeostasis by reducing intracellular current amplitudes; these pathways also act on sodium current, contributing to electrophysiological dysfunction. ²˒³ It was not possible to further investigate the BrS because the patient passed away. BrS could have explained the patient's symptoms (syncopes) in the absence of a prior cardiological history and family history of sudden cardiac death. Furthermore, the case shows how the association between Brugada Syndrome and sepsis represents a complex clinical condition, in which multiple triggers cause electrophysiological alterations of the heart inducing the onset of arrhythmias. 1.Carbone F et al. 2022. "Septic Cardiomyopathy: From Pathophysiology to the Clinical Setting" Cells 11, no. 18: 2833. 2. Zaky A. et al. Characterization of Cardiac Dysfunction in Sepsis: An Ongoing Challenge. Shock 41(1):p 12-24, January 2014. 3. Alain R. et al Early functional and transcriptomic changes in the myocardium predict outcome in a long-term rat model of sepsis. Clin Sci (Lond) 1 March 2013; 124 (6): 391–401.