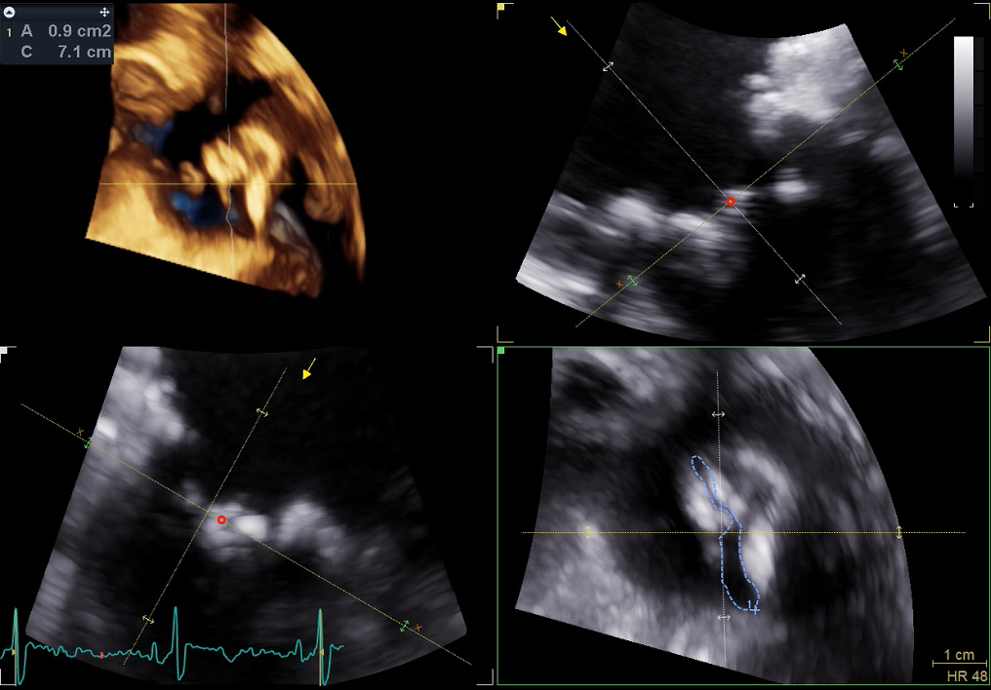
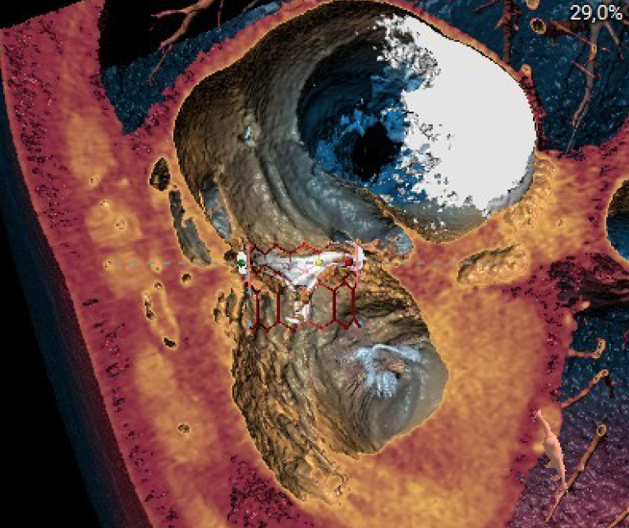
Degeneration of tricuspid bioprostheses represents a relevant clinical issue in patients with complex congenital heart disease, such as Ebstein’s anomaly, in whom redo cardiac surgery is associated with high morbidity and mortality. We report the case of a 75-year-old woman with Ebstein’s anomaly who had previously undergone double surgical tricuspid valve replacement with bioprostheses (1997 and 2011), referred to our center for progressive dyspnea and asthenia. Transthoracic echocardiography revealed severe stenosis of the tricuspid bioprosthesis, with a mean inspiratory gradient of 12 mmHg and moderate regurgitation, associated with right ventricular dysfunction. Three-dimensional transesophageal echocardiography confirmed thickened, partially fused and calcified leaflets, with reduced valve opening (planimetric area 0.9 cm²). Given the high surgical risk (STS score: 6.01% mortality, 18.9% morbidity; EuroSCORE II: 10.56%) and a favorable oncological prognosis (>12 months), the case was discussed by the Heart Team, which opted for a transcatheter tricuspid valve-in-valve (TVIV) procedure, after informed consent for off-label use. Pre-procedural planning with cardiac computed tomography and 3D reconstructions allowed accurate assessment of the prosthetic annulus. The procedure was successfully performed via transfemoral access using a 29-mm Edwards SAPIEN 3 Ultra RESILIA valve, implanted in reverse orientation under fluoroscopic guidance. Positioning of a stiff guidewire in the pulmonary artery proved crucial to ensure adequate system support in the presence of a small right ventricular cavity, typical of Ebstein’s anomaly. No procedural complications occurred. Post-implant echocardiography showed a mean tricuspid gradient of 1.7 mmHg, with no residual regurgitation or paravalvular leak. The patient experienced rapid clinical improvement, achieving NYHA functional class I, which was maintained at three-month follow-up with a normally functioning prosthesis. This case supports the feasibility, safety, and effectiveness of tricuspid valve-in-valve implantation in selected patients with complex anatomy due to Ebstein’s anomaly, highlighting the key role of multimodality imaging and procedural expertise.