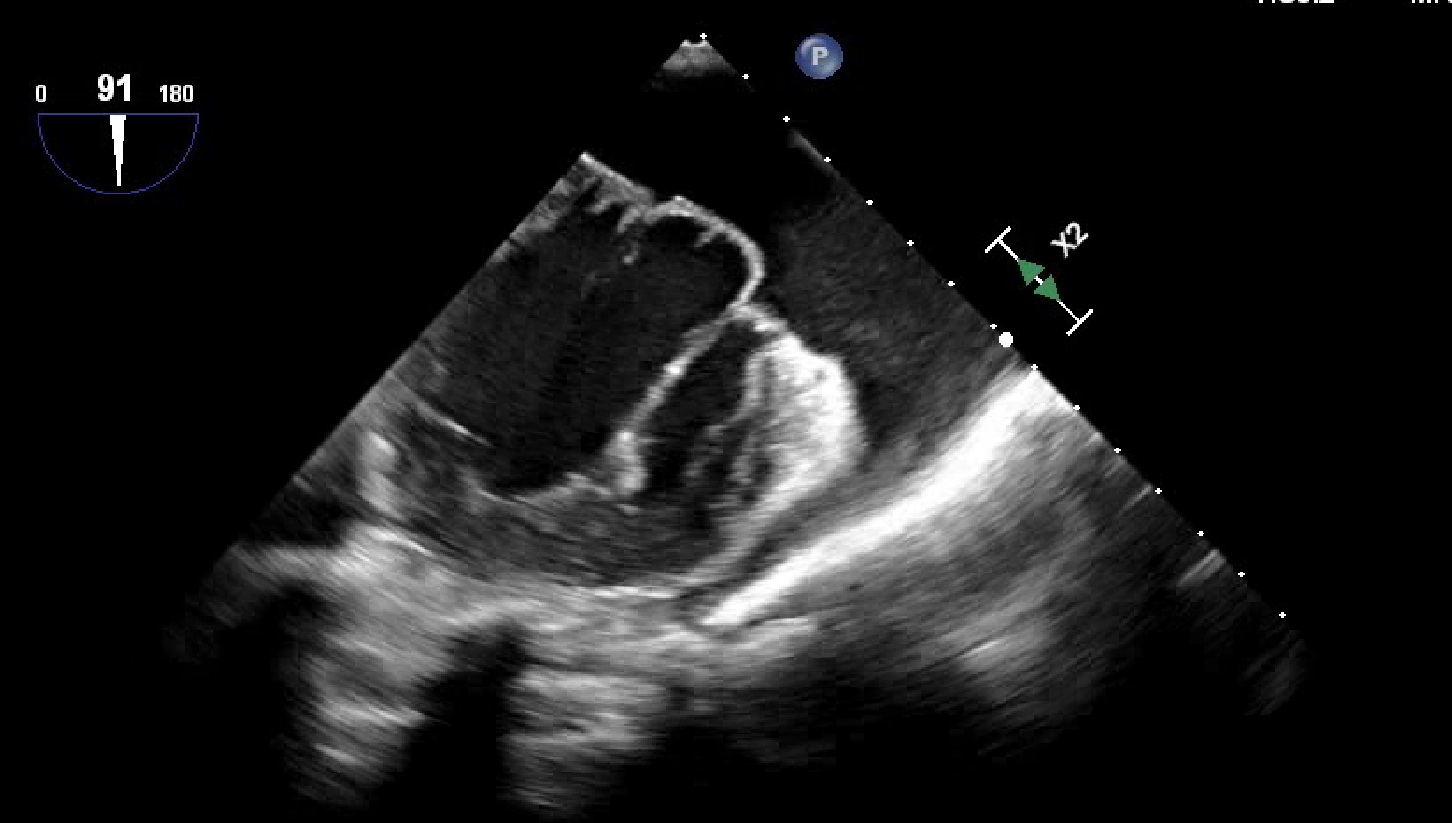
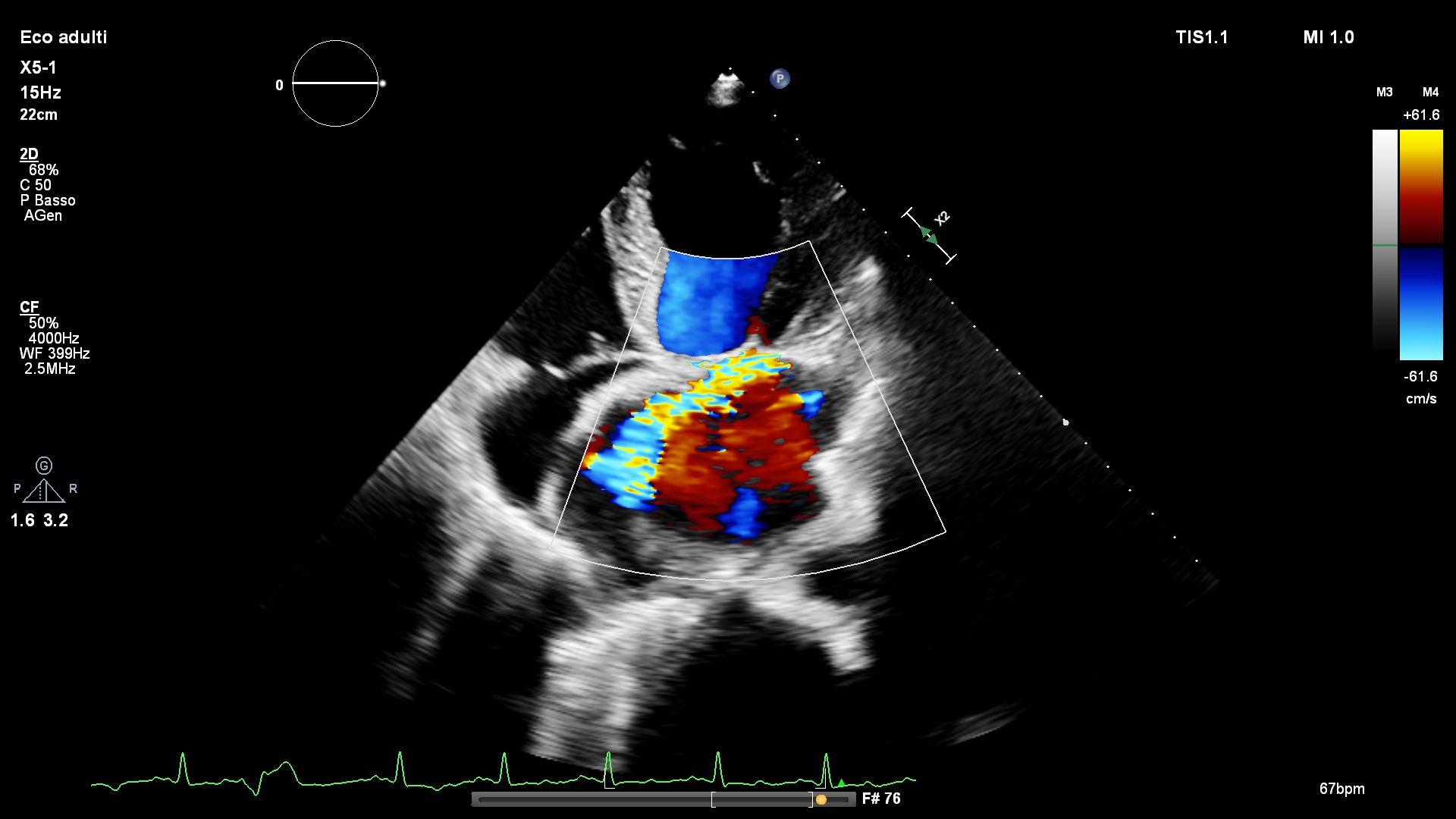
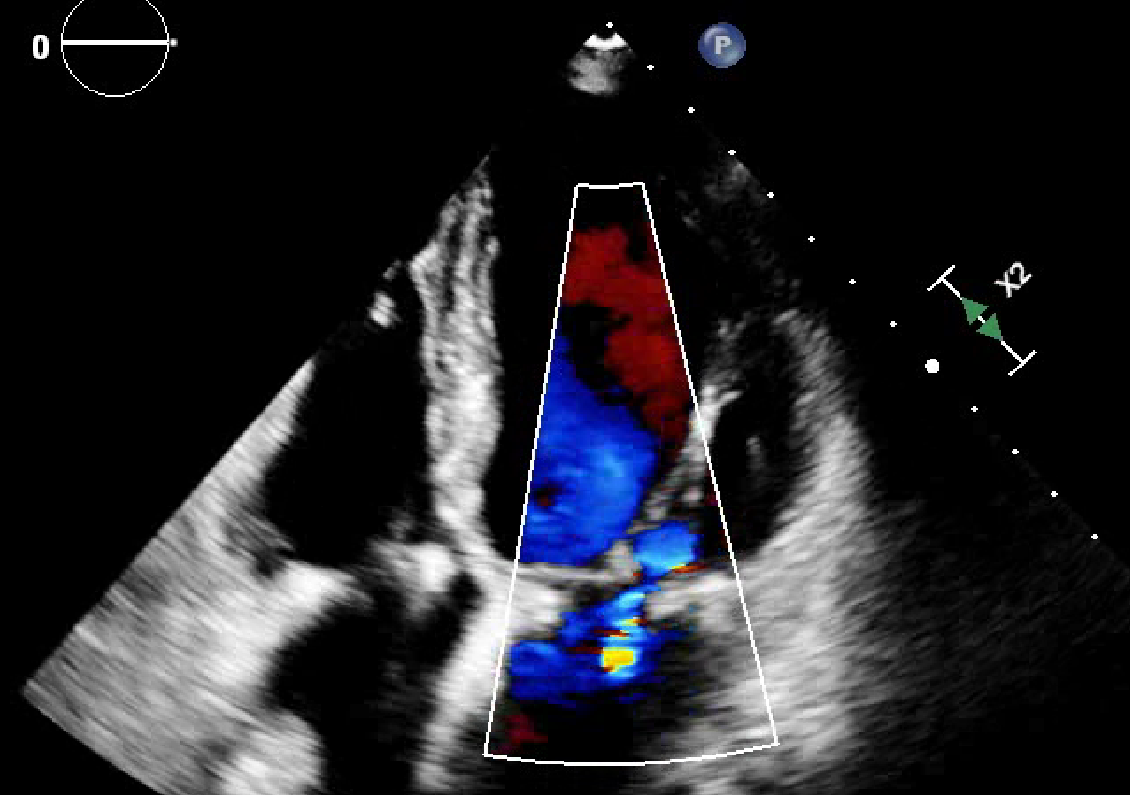
50-year-old female presented to the emergency department with acute heart failure. One month before, she had undergone mitral valvuloplasty (P1P2 prolapse) with implantation of a Physio Flex ring and Gore-Tex neochords on P2; tricuspid valvuloplasty and left atrial appendage closure. Pre-discharge echocardiography showed normal left ventricular size, preserved ejection fraction, residual mild mitral regurgitation, and mild tricuspid regurgitation. At presentation, her ECG revealed atrial fibrillation with a high ventricular rate of undetermined duration. Echocardiography demonstrated a severe reduction in left ventricular ejection fraction (LVEF, 30%), moderate MR, mild TR without significant prosthetic gradients and circumferential moderate pericardial effusion (25 mm) with signs of early hemodynamic compromise. The patient was admitted to our cardiology unit for inadequate pharmacological heart rate control. Diuretic therapy, glucocorticoids, and colchicine were initiated. Due to persistent hypotension and inadequate chronotropic control, electrical cardioversion was attempted but was unsuccessful. Therapy with sotalol and digitalis was progressively titrated, which, added to a reduction in pericardial effusion, achieved effective heart rate control. Coronary angiography excluded an ischemic etiology of HFrEF. After stabilization with HFrEF therapy, the patient was discharged wearing a life vest. At follow-up, echocardiography demonstrated significant recovery of left ventricular function (LVEF 50%), comparable to her immediate postoperative values. The notable finding in this case was the progressive decline in LVEF. Our hypothesis is that the decline in LVEF was primarily due to alterations in preload and afterload following mitral valve surgery. Before surgery, cardiac output was maintained by preload dependency and lower afterload. Post-surgery, increased afterload and reduced preload in addition to subclinical ventricular dysfunction result in temporary LVEF decline. While tachycardia-induced cardiomyopathy from uncontrolled AF was considered, the lack of LVEF recovery immediately following heart rate control argued against this diagnosis. This case highlights the importance of early mitral valve repair, performed before the onset of subclinical dysfunction and preload dependency. Comprehensive heart failure medical therapy is essential to optimize filling pressures, reduce afterload, and prevent adverse remodeling in the postoperative setting