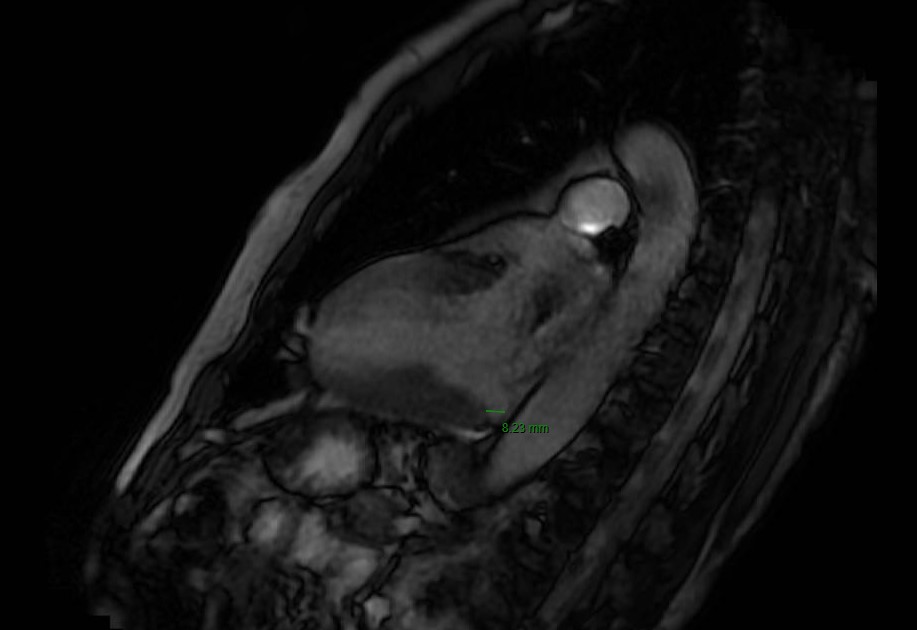
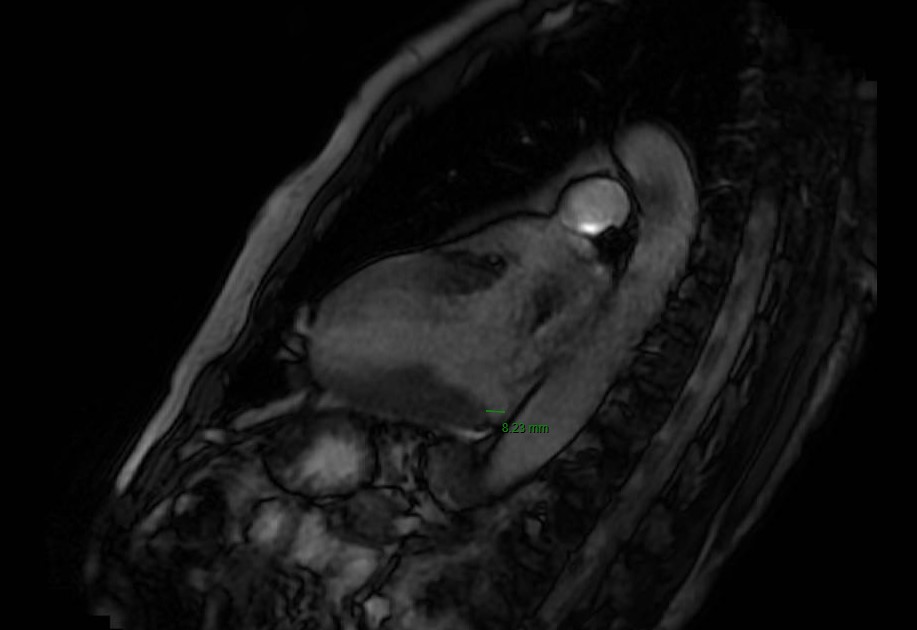
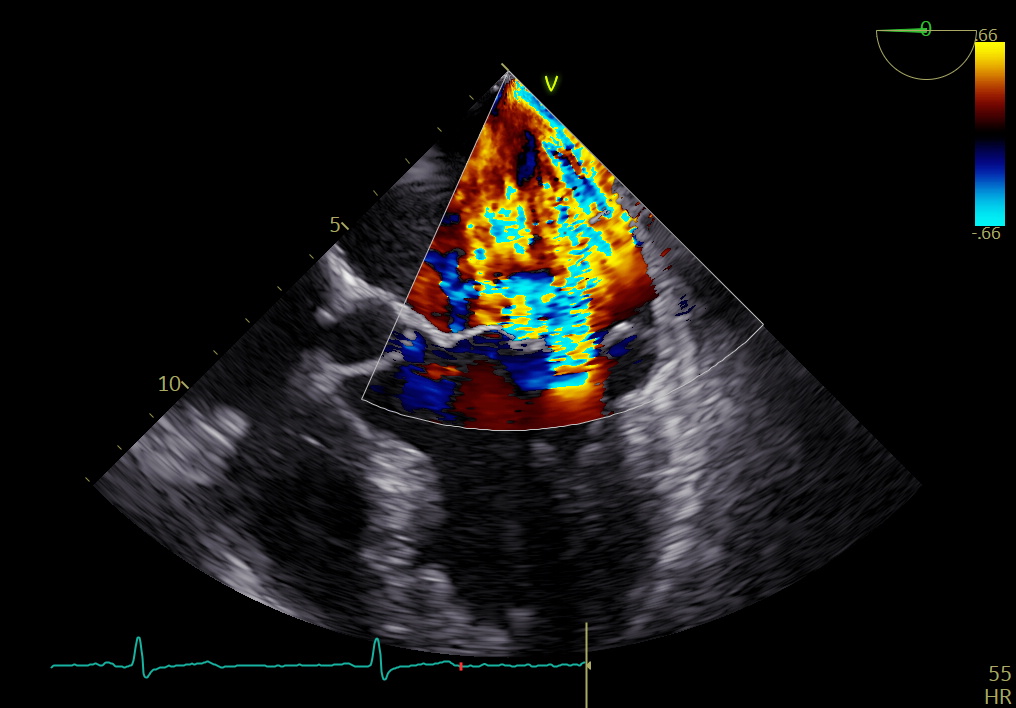
A 58-year-old man, heavy smoker with hypertension, presented with cardiac arrest with shockable rhythm. Emergency service was called and CPR started. DC shocks were administered with evidence of ROSC after 15 minutes. Orotracheal intubation was performed and the patient centralized to our emergency department. Total body CT scan excluded acute intracranial hemorrhages, PE and aortic dissection. The EKG after ROSC showed sinus rhythm with normal ventricular repolarization, the echocardiogram mild left ventricular dysfunction due to hypokinesia of apical septum and true apex. At coronary angiography diffuse ATS emerged with intermediate stenosis of the right coronary artery. Intraoperative TEE showed severe mitral valve insufficiency with multiple jets due to myxomatous and prolapsing leaflets without evidence of papillary muscles or chordal rupture. At ICU admission, the patient was sedated and mechanical ventilated, hemodynamically stable with MAP 90 mmHg, negative lactate on BGA. During the following 24 hours, he presented hypotension and hemodynamic instability, therefore dobutamine and norepinephrine were introduced and IABP positioned. Due to pulmonary congestion, endovenous diuretic was started. On the 4th day pharmacological support was progressively suspended and IABP removed. EKG monitoring did not show recurrences of ventricular arrhythmias. At neurological stratification EEG showed a favorable prognostic rhythm, good level of NSE, SSPE were within limits bilaterally but the neurological windows highlighted moments of agitation and a-purposeful movements. Due to the incomplete neurological recovery, on the 7th day percutaneous tracheostomy was performed and removed on the 22nd day after progressive weaning from ventilatory support. Cardiac MRI documented normal volumes and biventricular function with mitral prolapse, mitral annular disjunction of 8 mm and an area of intramyocardial DE with non-ischemic pattern of the basal infero-lateral wall. In light of the clinical presentation and the finding of arrhythmic mitral valve prolapse, the patient underwent S-ICD implantation. After a month of rehabilitation program with significant improvement of cognitive profile (CPC score 1-2), an ambulatory TEE was repeated. Severe multiple jet insufficiency due to malcoaptation was confirmed, with bi-leaflets prolapse more marked for P2 and a cleft between P1 and P2 in the absence of flail and chordal rupture. Indication for surgery correction was given.