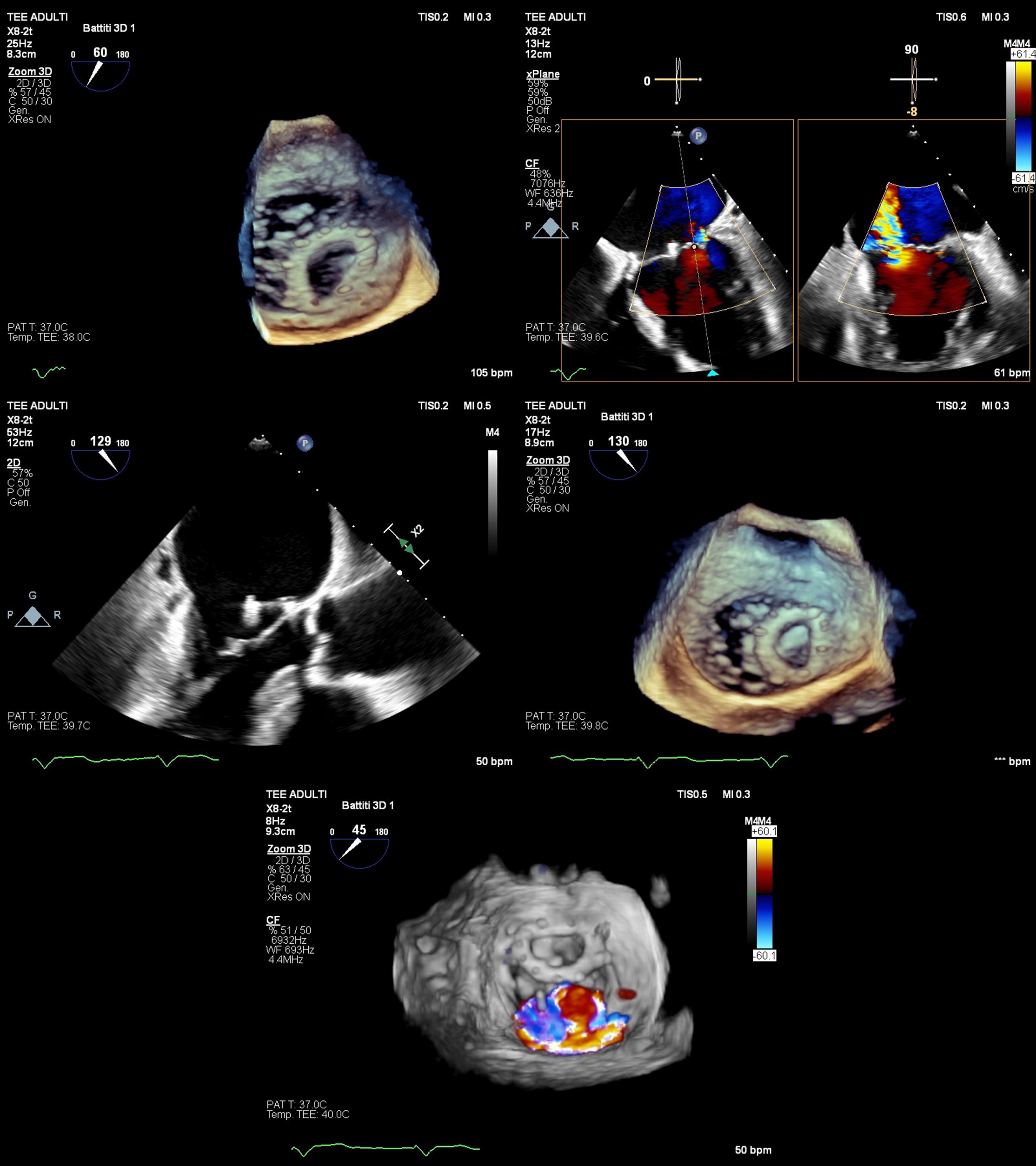
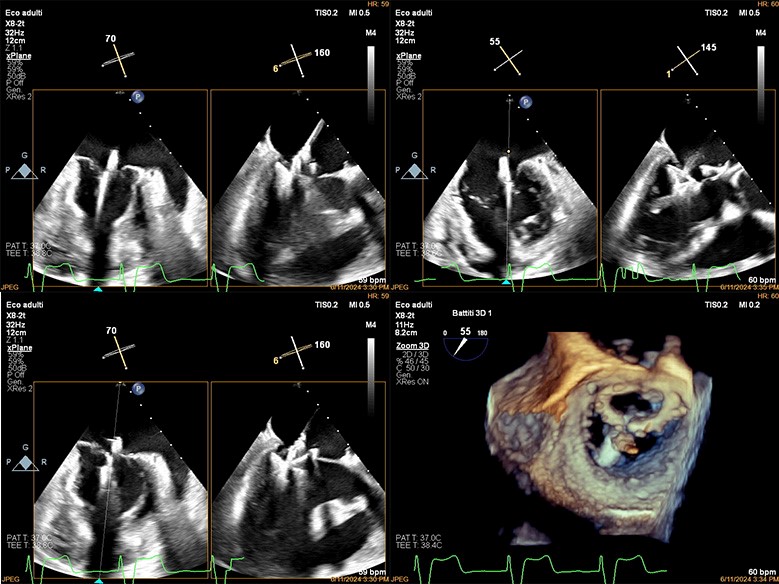
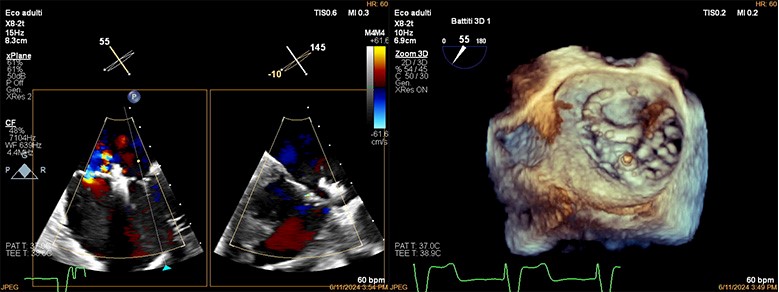
An 84-year-old male with no significant cardiovascular risk factors and a history of non-smoking was followed since 2012 for mild-to-moderate mitral regurgitation (MR) and tricuspid regurgitation. In 2014, he developed permanent bradycardic atrial fibrillation, necessitating implantation of a single-chamber pacemaker (VVI mode). By 2015, his condition progressed to severe MR of mixed etiology, with concentric left ventricular hypertrophy and an ejection fraction (EF) of 0.39. He underwent mitral valve repair with a Sorin Memo 3D annuloplasty ring. In June 2023, after a domestic accident caused a large hematoma on his right leg, anticoagulation therapy with a NOAC was temporarily suspended. Subsequent imaging revealed a penetrating ulcer in the common iliac artery and a 4.5 cm aneurysm in the right internal iliac artery, managed with an aorto-biiliac stent graft. A follow-up echocardiogram in July 2023 showed severe MR with an eccentric jet due to annuloplasty ring dehiscence, increased left ventricular end-diastolic volume (76 ml/m²), reduced EF (43%), and left atrial dilation (76 ml/m²). The Heart Team deemed the patient unsuitable for reoperation due to high surgical risk (STS Score), severe left ventricular dysfunction, and complex valve anatomy. A minimally invasive percutaneous mitral valve repair with the PASCAL Ace system was planned. The PASCAL Ace device was successfully implanted via transseptal puncture, anchoring the A2-P2 segments despite the dislocated annuloplasty ring. No complications arose, and the patient was discharged after six days. Post-procedure, MR was mild with a mean mitral gradient of 3.6 mmHg and effective valve area of 3.5 cm². At one and six months, the patient showed significant improvement: EF > 60%, residual MR 1+/4, and PAPs 35 mmHg. The patient resumed daily activities, including long-distance cycling, without fatigue or dyspnea. Current therapy includes furosemide, sacubitril/valsartan, empagliflozin, edoxaban, and other supportive medications. Anticoagulation remains essential due to atrial fibrillation.