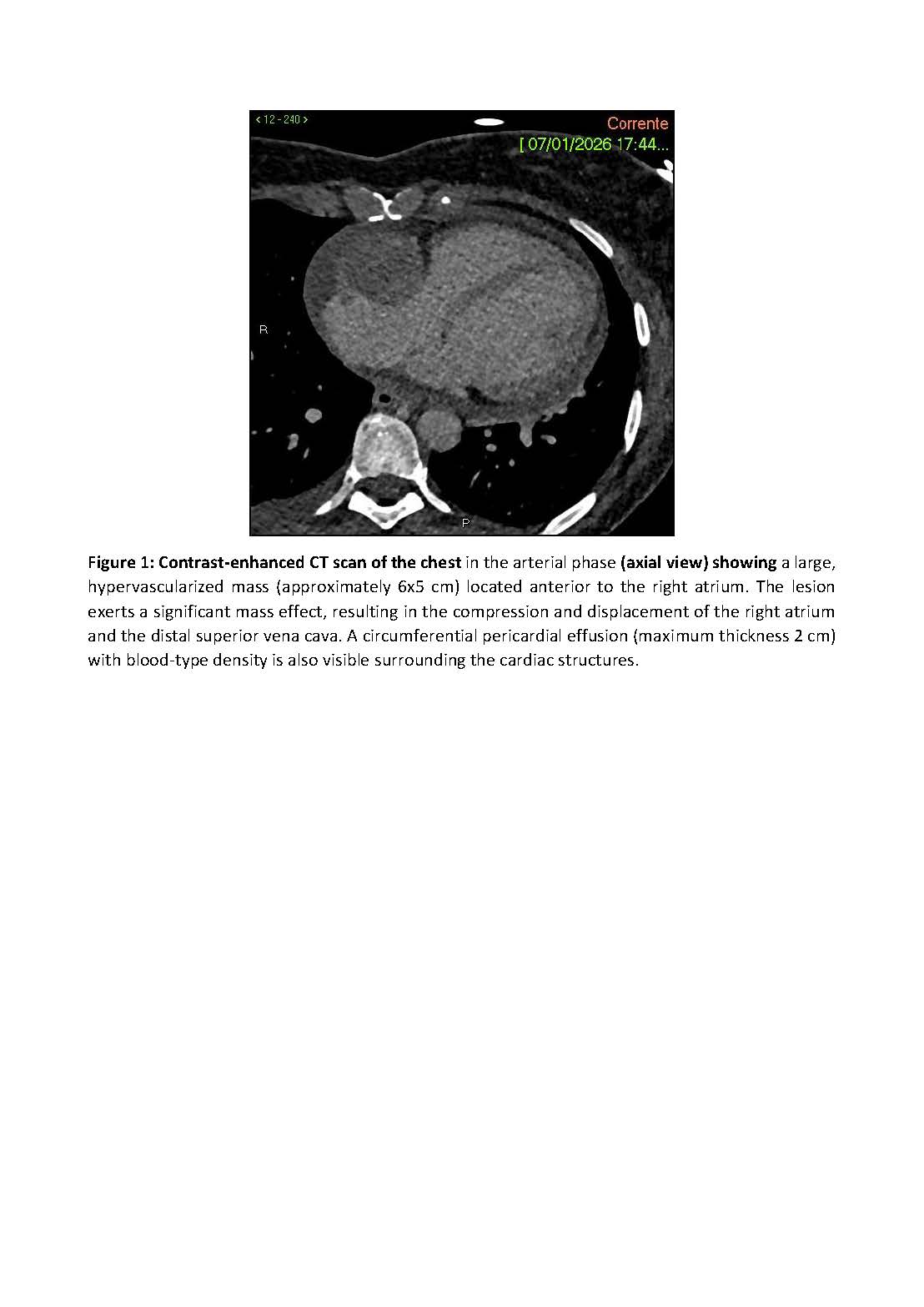
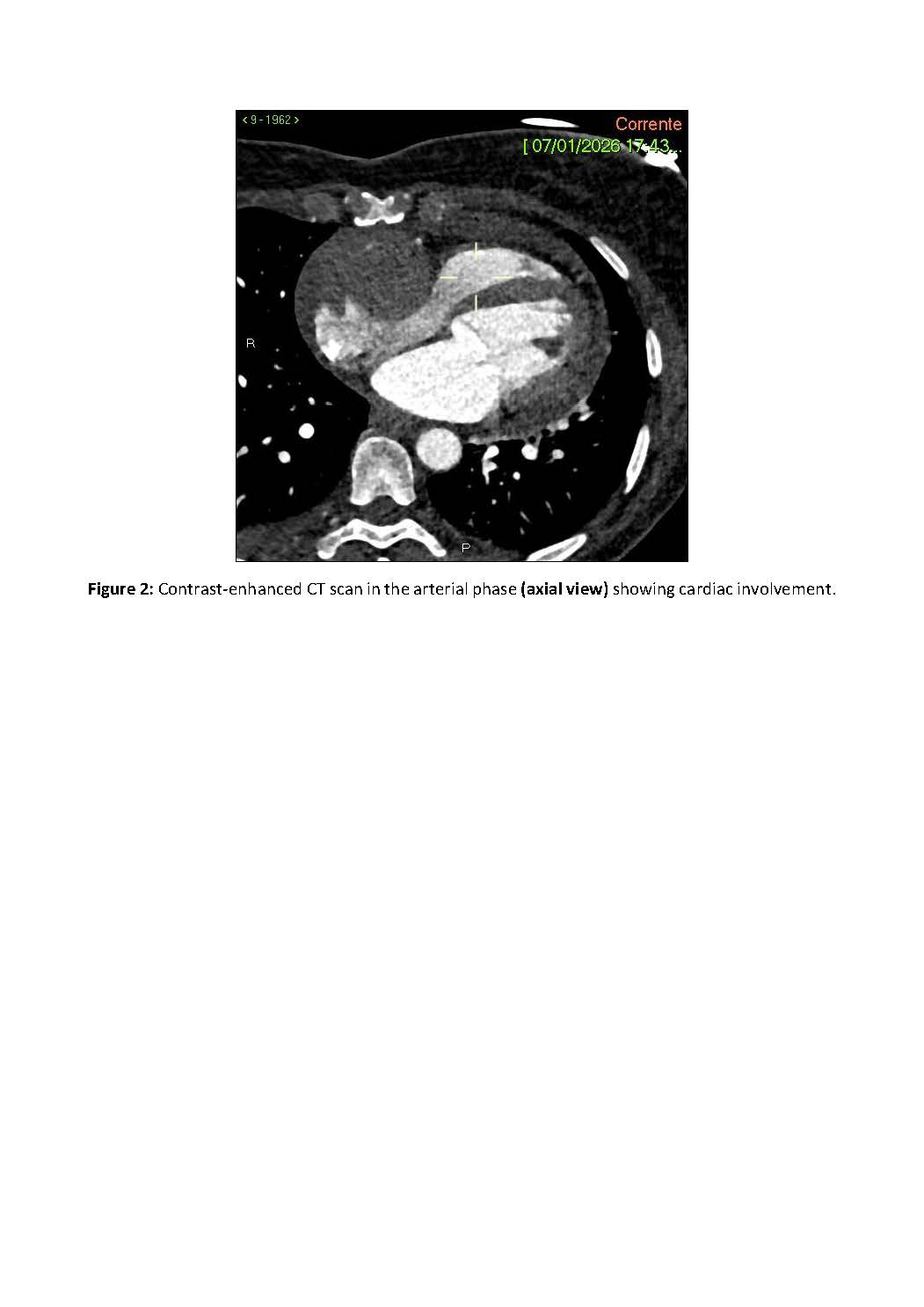
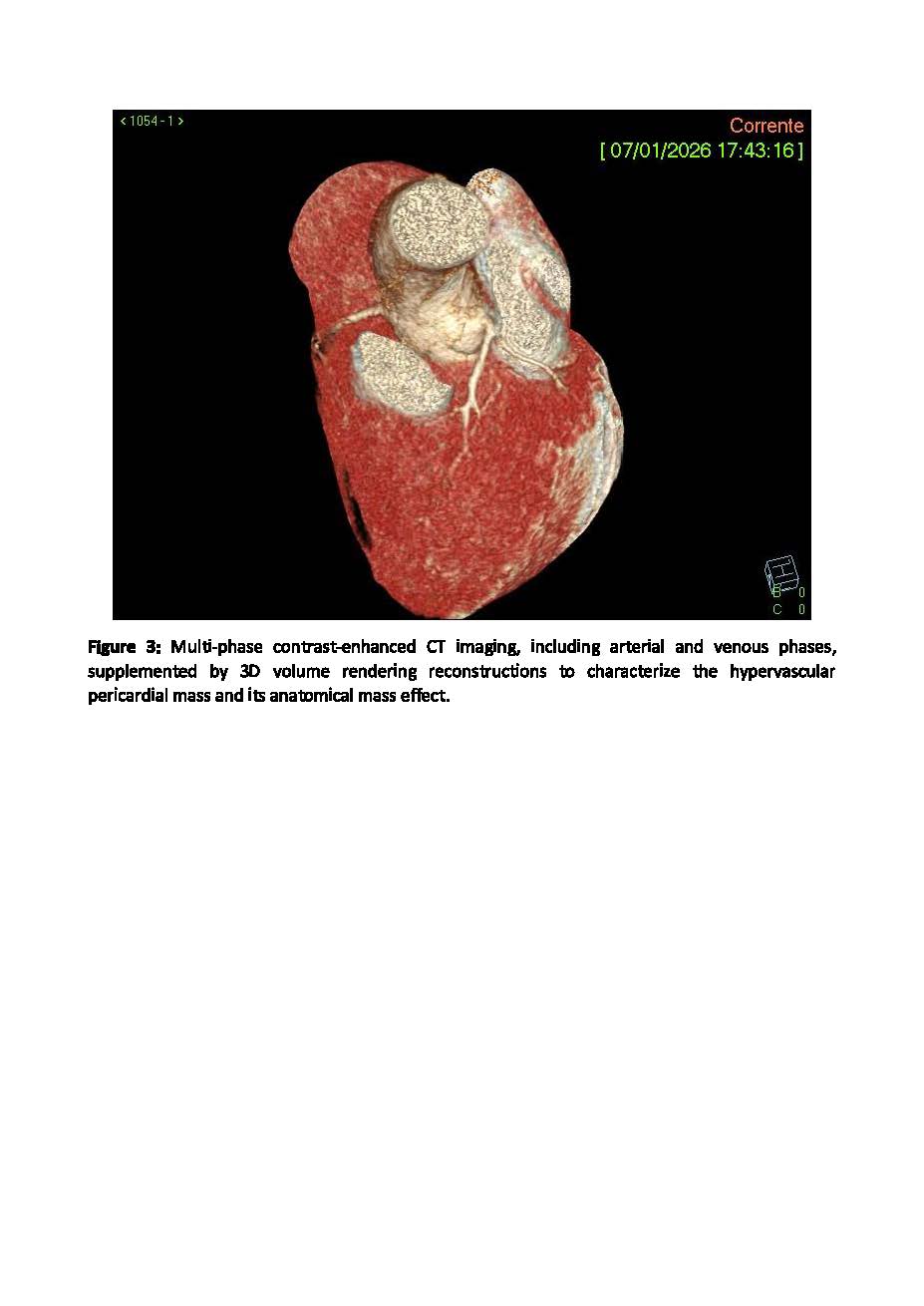
Background: Right atrial masses associated with pericardial effusion represent a rare but clinically relevant diagnostic challenge, requiring a multimodality imaging approach to differentiate between neoplastic, inflammatory, and infectious etiologies. Case Presentation A 56-year-old woman presented to the ED with progressive dyspnea for one month. In the week before admission, she reported flu-like symptoms with low-grade fever, asthenia, myalgia, and diarrhea. Her medical history was unremarkable. On examination, she appeared mildly distressed with tachypnea. Blood pressure was normal, heart rate mildly elevated, and oxygen saturation slightly reduced on room air. Cardiac auscultation revealed muffled heart sounds; lung examination was normal, and no peripheral edema was observed. Laboratory tests showed mildly elevated inflammatory markers with normal cardiac enzymes. TTE revealed a circumferential pericardial effusion without tamponade and preserved ventricular EF. Chest CT suggested a primary pericardial neoplasm, with hemangioendothelioma as the leading differential diagnosis, although secondary inflammatory involvement could not be excluded.. (Figure 1, 2 and 3). Discussion and Conclusions The coexistence of a right atrial mass and pericardial effusion posed a major diagnostic challenge. Differential diagnoses included primary cardiac tumors, metastatic disease, pericardial mesothelioma, and inflammatory or infectious conditions. Recent flu-like and gastrointestinal symptoms suggested a possible inflammatory trigger; however, a neoplastic etiology remained likely. This case highlights the importance of multimodality imaging in patients with unexplained systemic symptoms. Early identification of cardiac masses with pericardial involvement is essential for timely diagnosis and management.