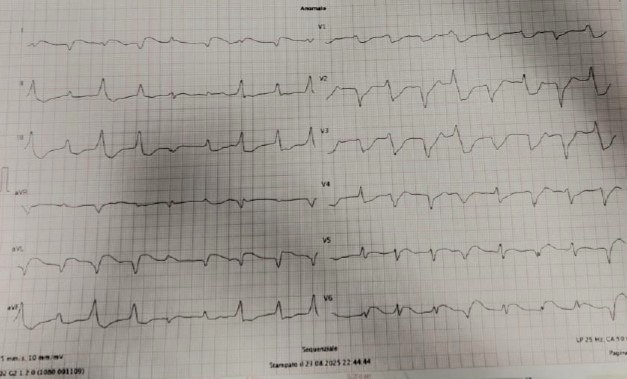
Myocarditis associated with immune checkpoint inhibitors (ICIs) is a rare complication but carries a high mortality rate. The clinical presentation can mimic acute coronary syndrome, making diagnosis complex and often delayed.An 81-year-old man was admitted to the emergency department with worsening dyspnea. The ECG showed lateral ST-segment elevation associated with a wide QRS complex, absent in previous tracings. The echocardiogram showed a severe reduction in global systolic function with akinesia of the lateral wall and apex, associated with bilateral pleural effusion. Blood tests showed a marked increase in myocardiokinecrosis enzymes. He had a history of squamous cell carcinoma of the scalp undergoing treatment with nivolumab. The patient was transferred to the intensive care unit and underwent urgent coronary angiography, which did not reveal any hemodynamically significant coronary stenosis.During his hospital stay, he experienced rapid clinical deterioration, culminating in cardiogenic shock. The patient was subjected to infusion therapy with norepinephrine and dobutamine at maximal doses with little benefit. Echocardiography showed a further reduction in ejection fraction with severe reduction in stroke volume (SVi 20 ml/min). In the absence of an ischemic cause and in light of ICI exposure, a diagnosis of checkpoint inhibitor-mediated immune myocarditis was made, and treatment with methylprednisolone was immediately initiated. Magnetic resonance imaging was not performed due to the patient's marked hemodynamic instability. The patient underwent BEM with evidence of a CD4- and CD8-positive lymphocyte infiltrate associated with myocardial necrosis, thus confirming the diagnosis of ICI-mediated myocarditis. Despite intensive care, the patient died of refractory cardiogenic shock. Myocarditis is characterized by a mortality rate exceeding 50%, representing a significant challenge in the Intensive Care Unit.