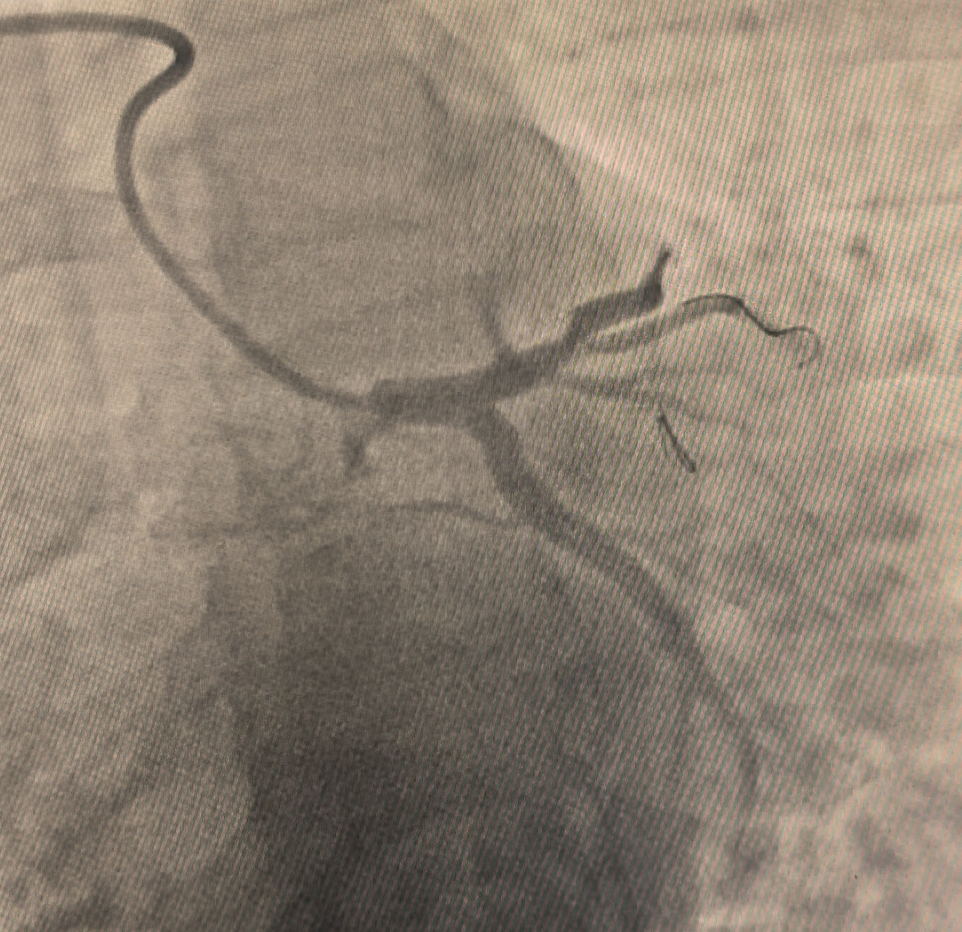
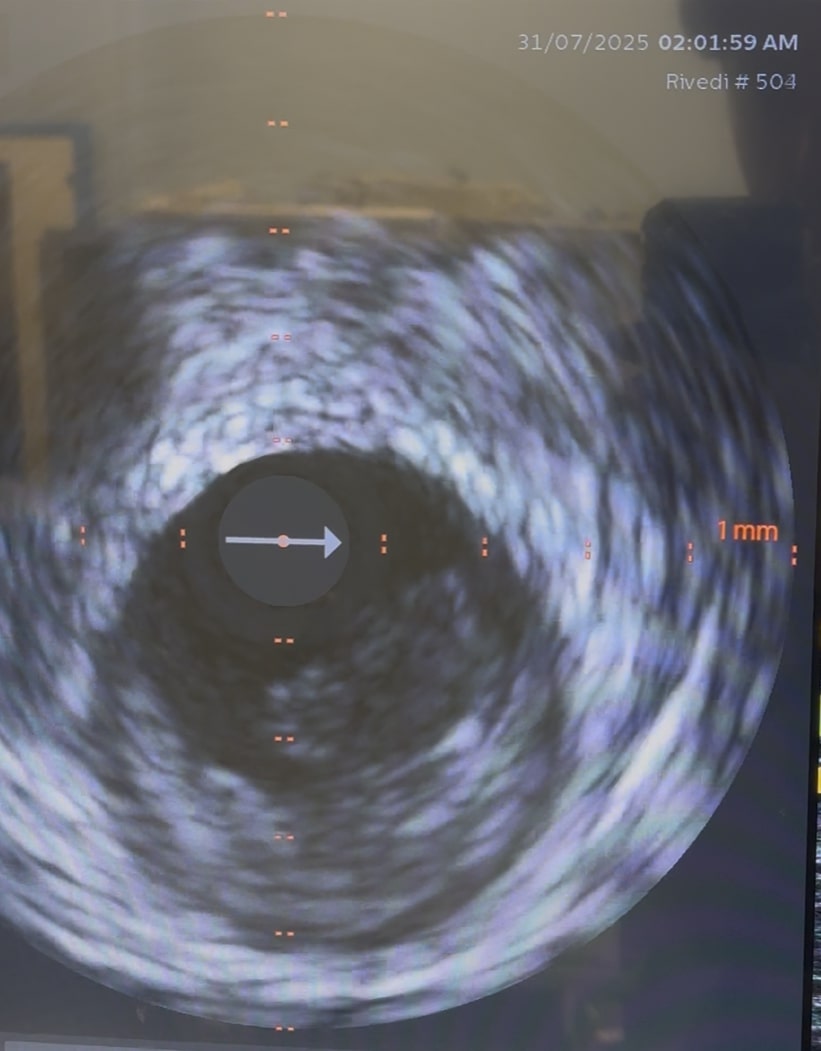
ST-elevation myocardial infarction (STEMI) in patients younger than 40 years represents a distinct clinical entity compared with ACS in older populations. In this age group, traditional atherosclerotic mechanisms driven by long-standing exposure to classical cardiovascular risk factors are less prevalent, while alternative or overlapping pathophysiological processes play a more prominent role. These include plaque erosion, isolated coronary thrombosis, spontaneous coronary artery dissection, vasospasm, and inherited or acquired pro-thrombotic conditions. In the present case, intravascular ultrasound (IVUS) demonstrated a non-calcified atherosclerotic plaque with endothelial erosion and superimposed thrombus, without evidence of plaque rupture or dissection. Plaque erosion is increasingly recognized as a frequent substrate of ACS in young patients, particularly smokers, and is characterized by endothelial denudation, preserved fibrous cap integrity, and high thrombogenic potential. Smoking and acute physical exertion likely acted as triggers by promoting endothelial dysfunction, increased shear stress, and platelet activation. However, these factors alone may not fully explain the occurrence of myocardial infarction at such a young age. The identification of multiple pro-thrombotic genetic polymorphisms affecting fibrinolysis and the renin–angiotensin system suggests a permissive biological background favoring thrombus formation and persistence. Although each variant confers only a modest increase in cardiovascular risk, their coexistence may create a cumulative pro-inflammatory and pro-coagulant vascular milieu, facilitating early atherothrombosis even in the absence of dyslipidemia, metabolic syndrome, or autoimmune disease. This case underscores the importance of a comprehensive etiologic evaluation in young patients with STEMI. While current guidelines do not recommend routine thrombophilia screening in all ACS patients, such recommendations are largely derived from older populations. In patients under 40 years of age—especially those with few conventional risk factors or atypical angiographic findings—a more extensive diagnostic approach appears justified. Systematic use of intravascular imaging and selective genetic and thrombophilia testing in this population may improve understanding of disease mechanisms, refine risk stratification, and support more personalized long-term prevention strategies.