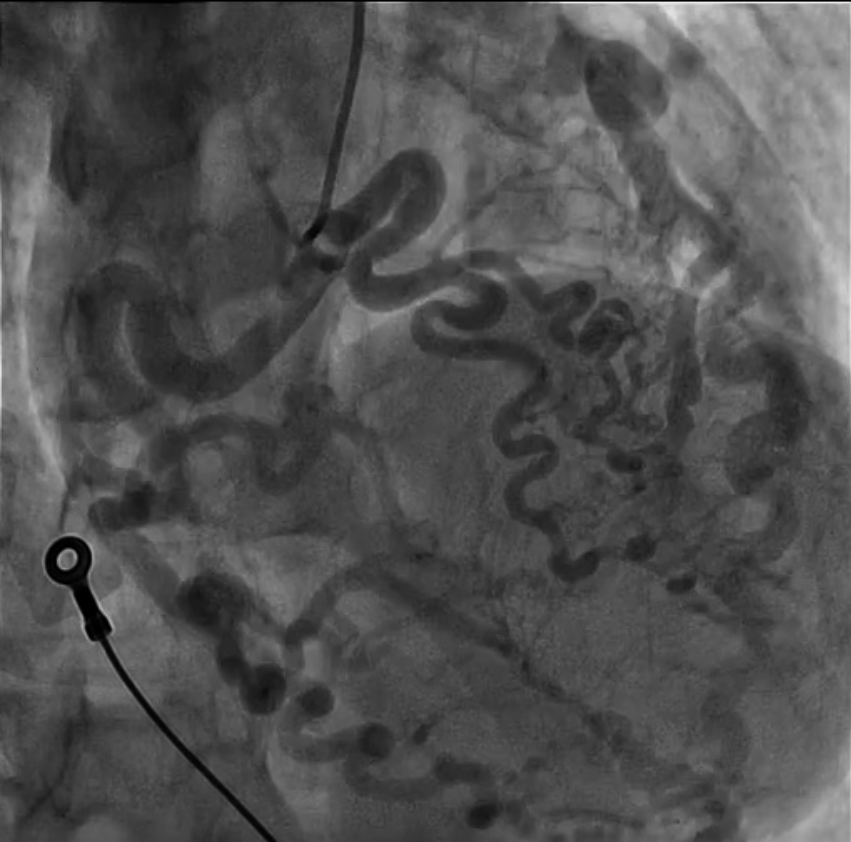
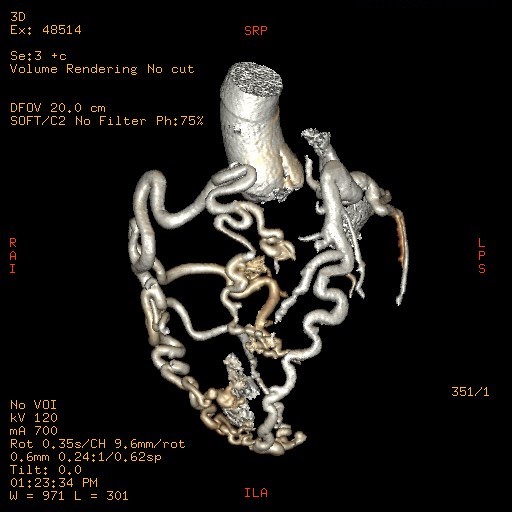
Background Out-of-hospital cardiac arrest is a major cause of mortality, most commonly related to ischemic heart disease. Rare congenital coronary anomalies may represent an uncommon but potentially lethal substrate for malignant ventricular arrhythmias. Case Presentation A 42-year-old woman with no known cardiovascular history was found unconscious in an out-of-hospital setting. On arrival of Emergency Medical Services, she was in cardiac arrest due to ventricular fibrillation. Electrical defibrillation restored spontaneous circulation(ROSC). Post-ROSC EKG showed a new-onset left bundle branch block. Urgent coronary angiography revealed a complex congenital coronary anomaly characterized by absence of the left main coronary artery and a single coronary artery arising from the right coronary sinus. The vessel appeared markedly ectatic and tortuous, giving rise to both the left anterior descending(LAD) and circumflex(LCx) arteries, without angiographically significant stenoses. Multiple coronary arteriovenous fistulas draining into the pulmonary artery and involving septal branches were also observed ( Image 1A ). Coronary CT confirmed the absence of the left main coronary artery and demonstrated a single ectatic coronary artery (up to 7 mm) originating from the right coronary sinus, with a highly tortuous course and formation of a vascular network at the cardiac apex. Retrograde filling of a dilated LAD and origin of a dilated LCx (7–8 mm) were observed ( Image 1B-C ). Multiple fistulous connections with hypertrophic bronchial arteries were present. A right-sided pneumothorax and pneumomediastinum were also detected and successfully treated with chest drainage. After a few days in the intensive care unit, the patient was weaned from mechanical ventilation with complete neurological recovery. Initial transthoracic echocardiography showed severe left ventricular systolic dysfunction (LVEF 30–35%), which improved to 60% during hospitalization. Given the occurrence of ventricular fibrillation in the absence of a reversible ischemic cause, a dual-chamber implantable cardioverter-defibrillator was implanted for secondary prevention. At discharge, the patient was prescribed only a beta-blocker. Conclusion This case highlights a rare presentation of complex congenital coronary artery anomaly with extensive coronary fistulization leading to sudden cardiac arrest. Advanced imaging and multidisciplinary management were essential for diagnosis and favorable outcome.