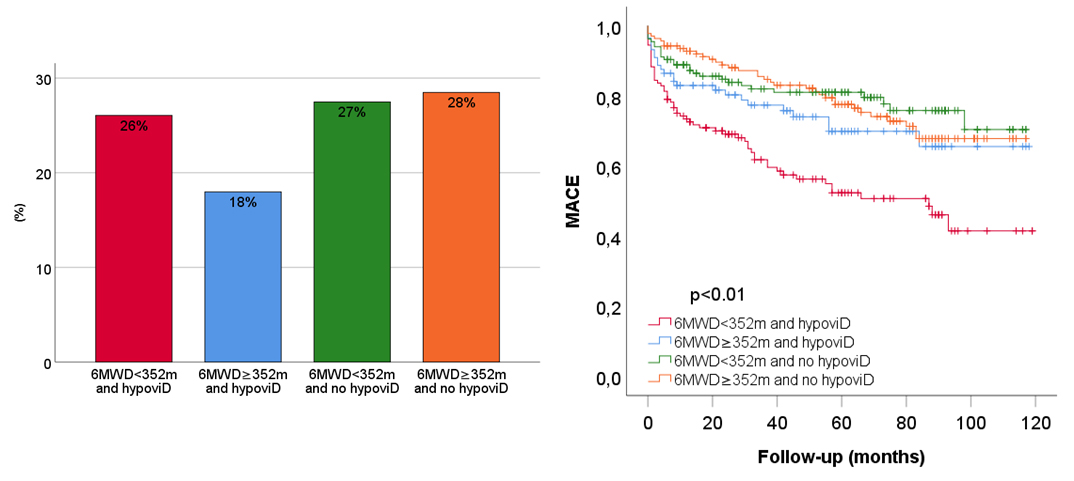
Background: The six-minute walk test (6MWT) reliably assesses exercise capacity of patients. Vitamin D influences muscle strength and function promoting protein synthesis and regulating calcium and phosphate levels. Purpose: To evaluate the relationship between hypovitaminosis D levels and 6MWT results, and their prognostic significance in patients with acute myocardial infarction (AMI). Methods: Blood samples were collected from 498 patients. Levels of vitamin D≤20 ng/ml was defined as hypovitaminosis D. The combined endpoint comprised all-cause mortality, re-infarction, and heart failure development. Results: The mean age of the cohort was 64 years, with 79% being male and 86% presenting with STEMI. The median vitamin D level was 19 [12.1–25.8] ng/ml, and 54% of patients had hypovitaminosis D. Before discharge, patients underwent a 6MWT with dyspnea assessed using the Borg CR10 scale. Most reported absent/mild dyspnea (Borg 0–2), while one-quarter had moderate/severe dyspnea (Borg 3–10). The mean 6-minute walk distance (6MWD) was 352±83 m. Patients with hypovitaminosis D have significantly lower 6MWD compared to those without (340±83 m Vs 364±81 m, p<0.01, respectively). At binary logistic regression analysis, lower 6MWD was predicted by older age, female gender, higher BMI, lower vitamin D levels and worse left ventricular ejection function (LVEF), after correction for smoking, diabetes and Borg scale. Patients were grouped by 6MWD and vitamin D level: Group 1 (low 6MWD, hypovitaminosis D), Group 2 (high 6MWD, hypovitaminosis D), Group 3 (low 6MWD, no hypovitaminosis D), and Group 4 (high 6MWD, no hypovitaminosis D), (Fig. 1). Over a mean 48-month follow-up, 146 patients (29%) reached the composite endpoint. Kaplan-Meier analysis revealed a significantly higher risk of reaching the endpoint in Group 1 compared to the other groups (p<0.01) (Fig. 1). Cox regression confirmed that low 6MWD and hypovitaminosis D are independent predictors of adverse outcome (HR: 2.23, p<0.01), along with worse NHYA class, reduced LVEF, smoking and hypertension, adjusted for age, gender, diabetes, renal function and STEMI diagnosis. Conclusion: A shorter 6MWD was linked to hypovitaminosis D, with both factors associated with over a two-fold increase in adverse outcomes in AMI patients, alongside traditional risk factors. The 6MWT helps identify high-risk patients for CR programs, while vitamin D optimization may serve as an effective preventive strategy.