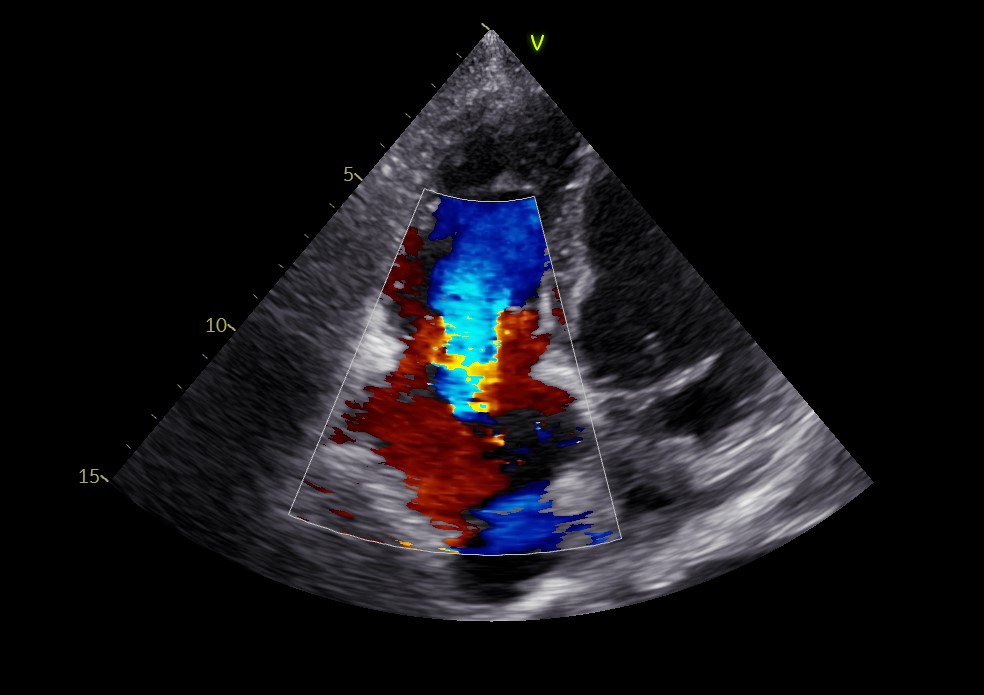
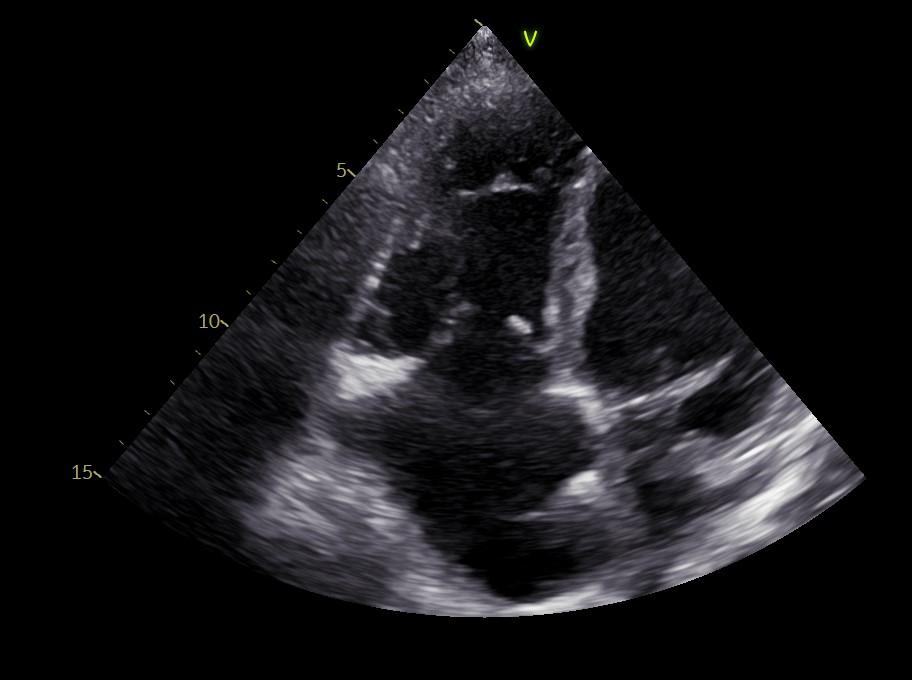
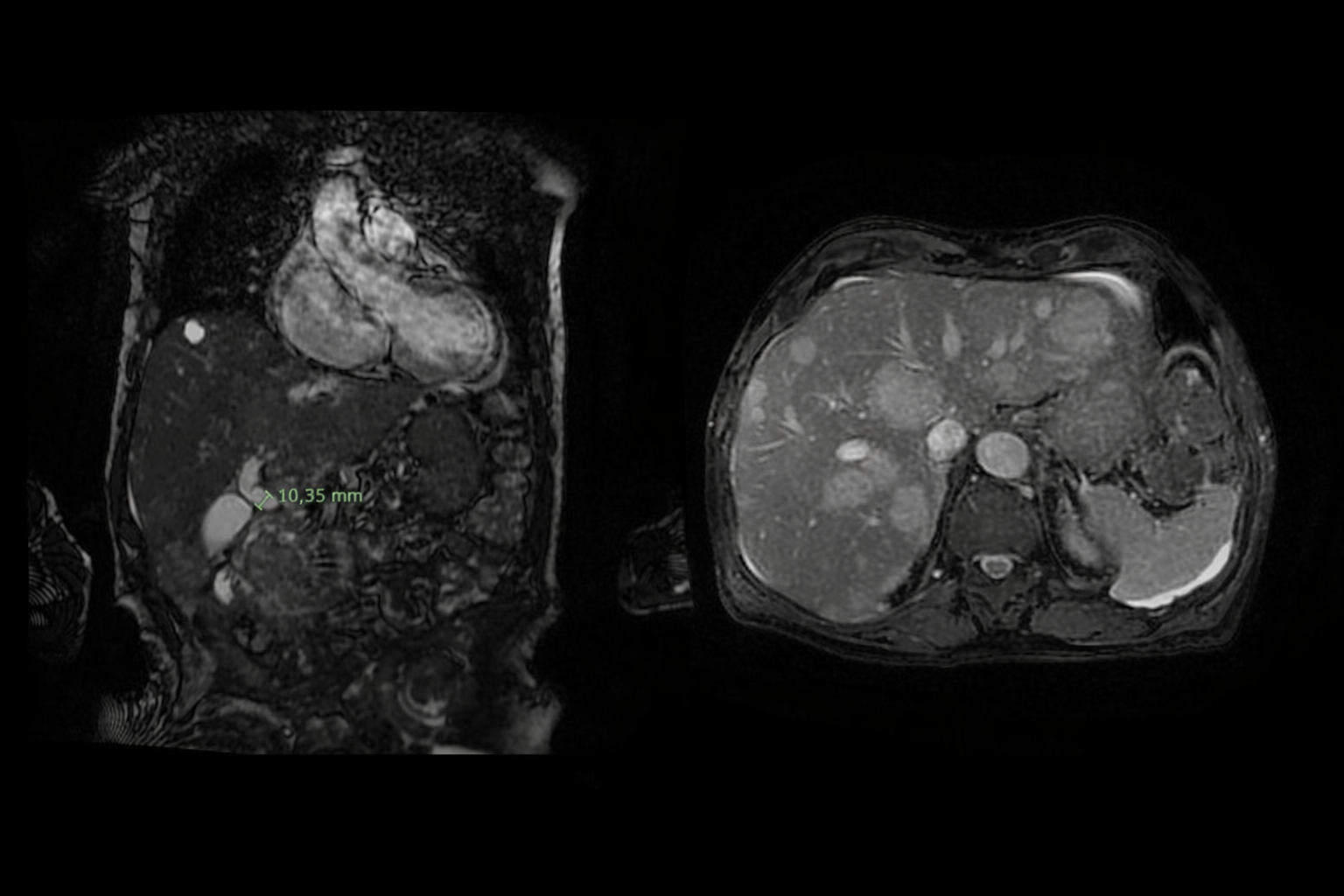
Introduction Carcinoid syndrome is a rare clinical condition caused by the systemic release of bioactive substances from a specific type of neuroendocrine tumors (NET) most commonly originating in the gastrointestinal tract. The syndrome typically develops during advanced or metastatic disease, particularly when hepatic involvement allows these vasoactive substances to bypass hepatic metabolism and enter the systemic circulation. Clinical case A 78 years-old man with a story of previous inferior-lateral myocardial infarction and paroxysmal atrial fibrillation came to our attention after the echocardiographic finding of severe tricuspid regurgitation, not present 6 months before, and associated with signs of right heart failure. EKG revealed atrial fibrillation, HR 89, Q wave in inferior leads. Echocardiography confirmed a severe tricuspid regurgitation, showing retracted and fibrotic tricuspid flaps, with large coaptation deficit (figure 1 and 2 ); right ventricle was dilated with preserved contractile function, left ventricle presented normal function. An Angio-CT of the chest showed no pulmonary embolism but a massive hepatic replacement by repetitive hypervascular lesions, associated with Wirsung’s duct dilatation, caused by the presence of a just partially visible cephalopancreatic mass. A MR-cholangiopancreatography confirmed these abdominal findings ( figure 3 ), suggesting a neuroendrocrine nature. To differentiate pancreatic adenocarcinoma from a NET, an ultrasound-guided biopsy was performed which identified a well-differentiated NET (G1) with molecular positivity for chromogranin and synaptophysin. Staging CT did not reveal any secondary lesions other than the liver but, due to the advanced hepathic dysfunction, the patient was considered unsuitable for surgical treatment of the valve and, after high-dose diuretic therapy, treatment with somatostatin analogues was started. Discussions In carcinoid syndrome, cardiac involvement is caused by the deposition of carcinoid fibrotic plaques on the right heart chambers and valves, which are the first structures to receive hormonal input from the circulation. Although the primary treatment for tricuspid valve dysfunction is surgery, when liver metastases from NET are so extensive, primary treatment of the underlying tumor remains essential, along with symptomatic therapy, to improve quality of life and control peripheral congestion.