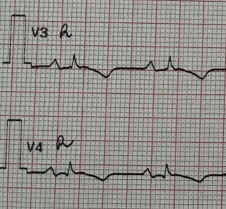
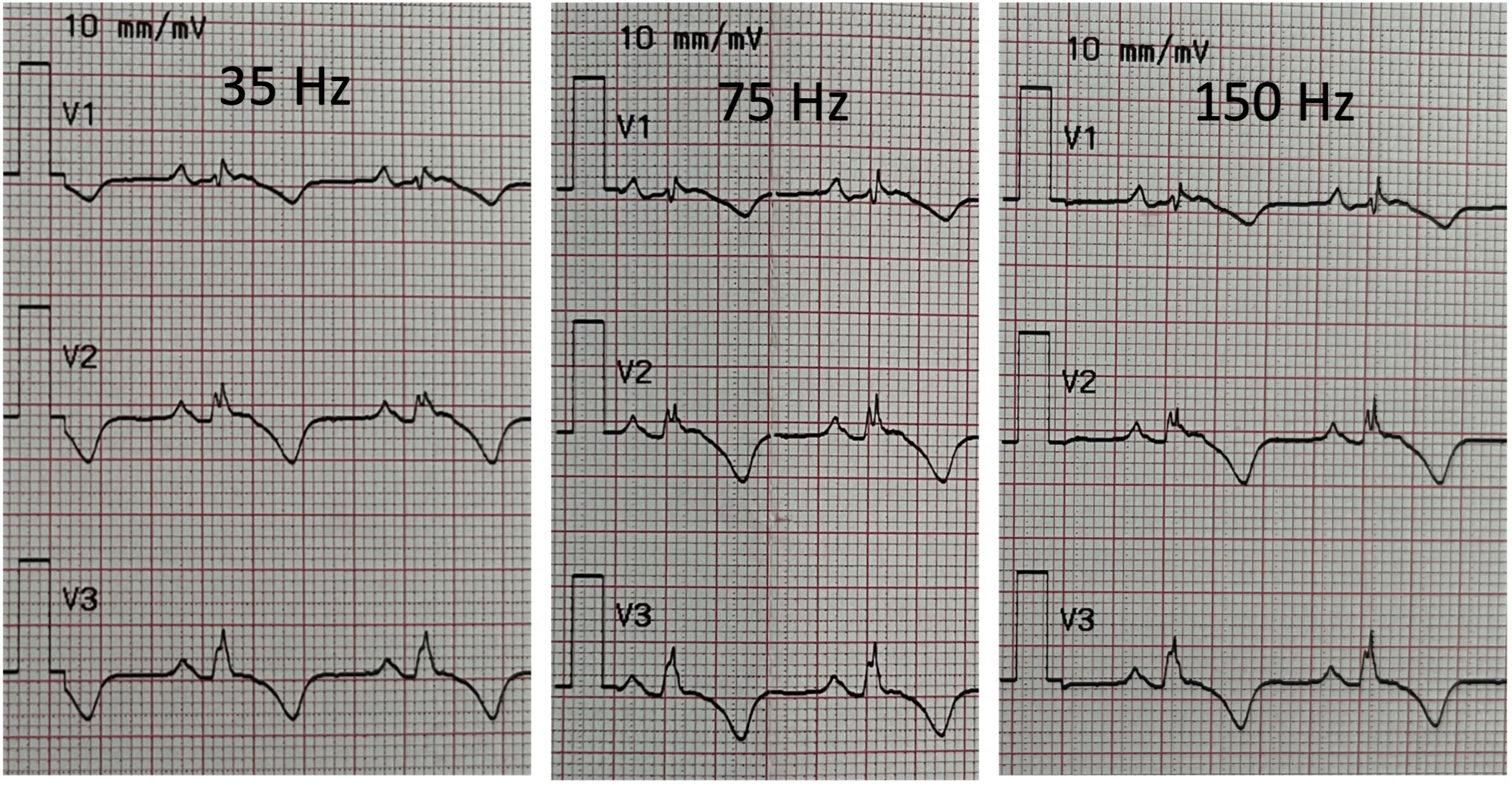
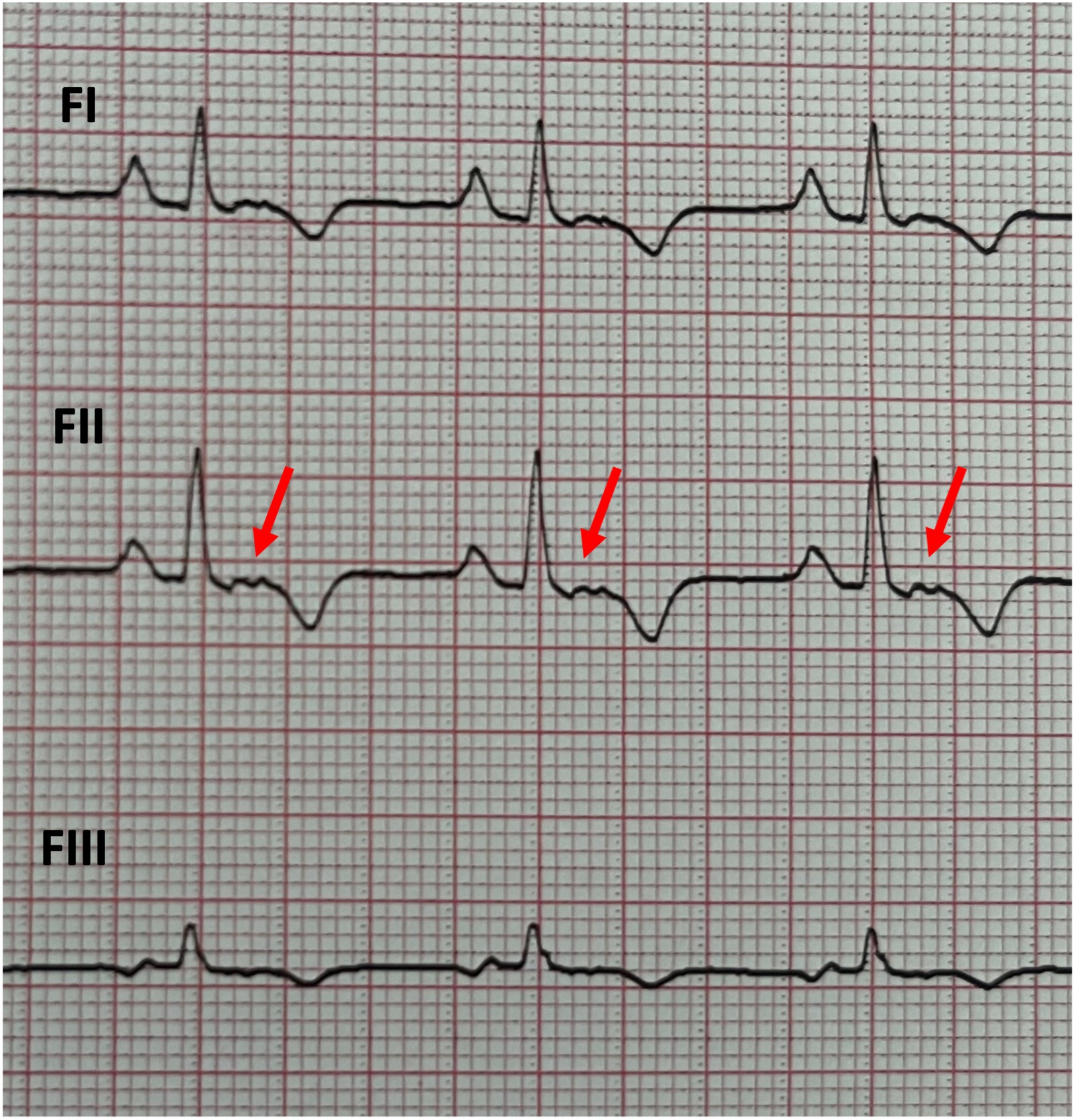
Background Depolarization abnormalities represent traditional electrocardiographic (ECG) criteria to diagnose arrhythmogenic right ventricular cardiomyopathy (ARVC). Given the challenges in their reliable detection, the diagnostic significance of epsilon waves has been downgraded to a minor criterion by the European Task Force in 2024. We present a case where the application of specific technical adjustments during ECG recording allowed of identification of epsilon waves, that were not evident on the baseline ECG. Case presentation A 56-year-old male patient, listed for heart transplant due to advanced plakophilin-2 ( PKP2 )-related ARVC, was admitted to our hospital for a ventricular tachycardia (VT) electrical storm, treated with correction of potassium imbalance, left stellate ganglion block, and antiarrhythmic drugs. Despite significant right ventricular dilation and dysfunction, the baseline ECG did not show clear epsilon waves. Their identification had no direct implications, however further technical adjustments were applied to unmask the presumed right ventricular depolarization abnormalities for speculative purposes. A standard 12-lead ECG with different low-pass filter settings was acquired (i.e., 35 Hz, 75 Hz, and 150 Hz – Figure 1), but no evident epsilon waves were documented. ECG recording from right precordial leads (V4R: fifth intercostal space along the right mid-clavicular line; V3R: midway between V1 and V4R – Figure 2) showed no trace of these waves. Consequently, Fontaine bipolar precordial leads (F-ECG) were acquired with the right arm electrode positioned on the manubrium, the left arm electrode over the xiphoid process, and the left leg electrode in the standard V4 position, creating F-ECG with FI, FII, FIII leads. This arrangement is used to specifically record potentials developed by delayed right ventricular fibers, covering the infundibulum, the apex, and the diaphragmatic surface of the right ventricle. FII revealed clear and reproducible epsilon waves (Figure 3). Conclusions This case suggests that epsilon wave remains a fundamental hallmark of the 'arrhythmogenic substrate' in ARVC. When standard 12-lead ECG and right-sided leads fail to reveal these signals, the use of Fontaine leads can unmask concealed depolarization abnormalities. Such procedural refinements enhance the sensitivity of surface ECG, confirming that the absence of evidence is not necessarily evidence of absence in complex cardiomyopathies.