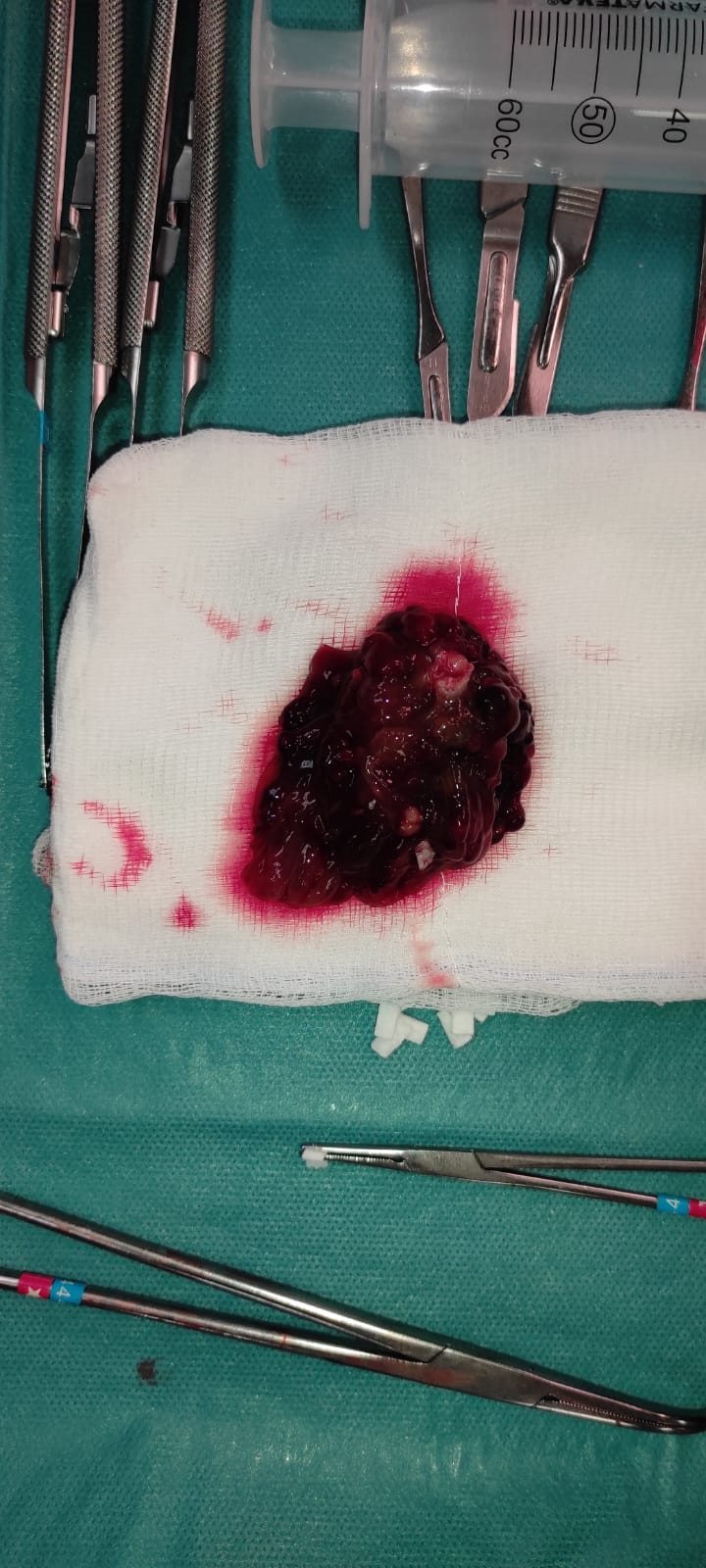
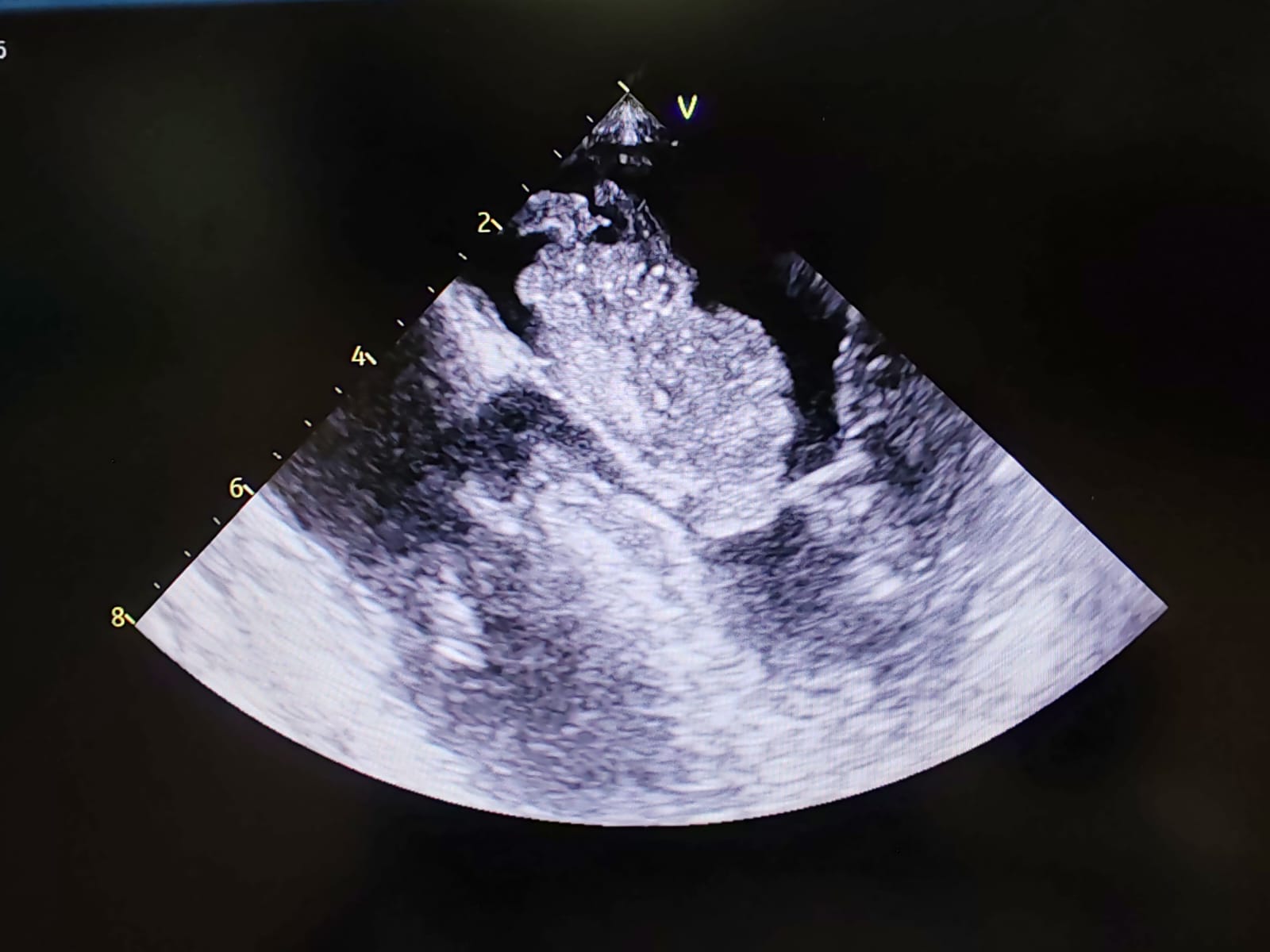
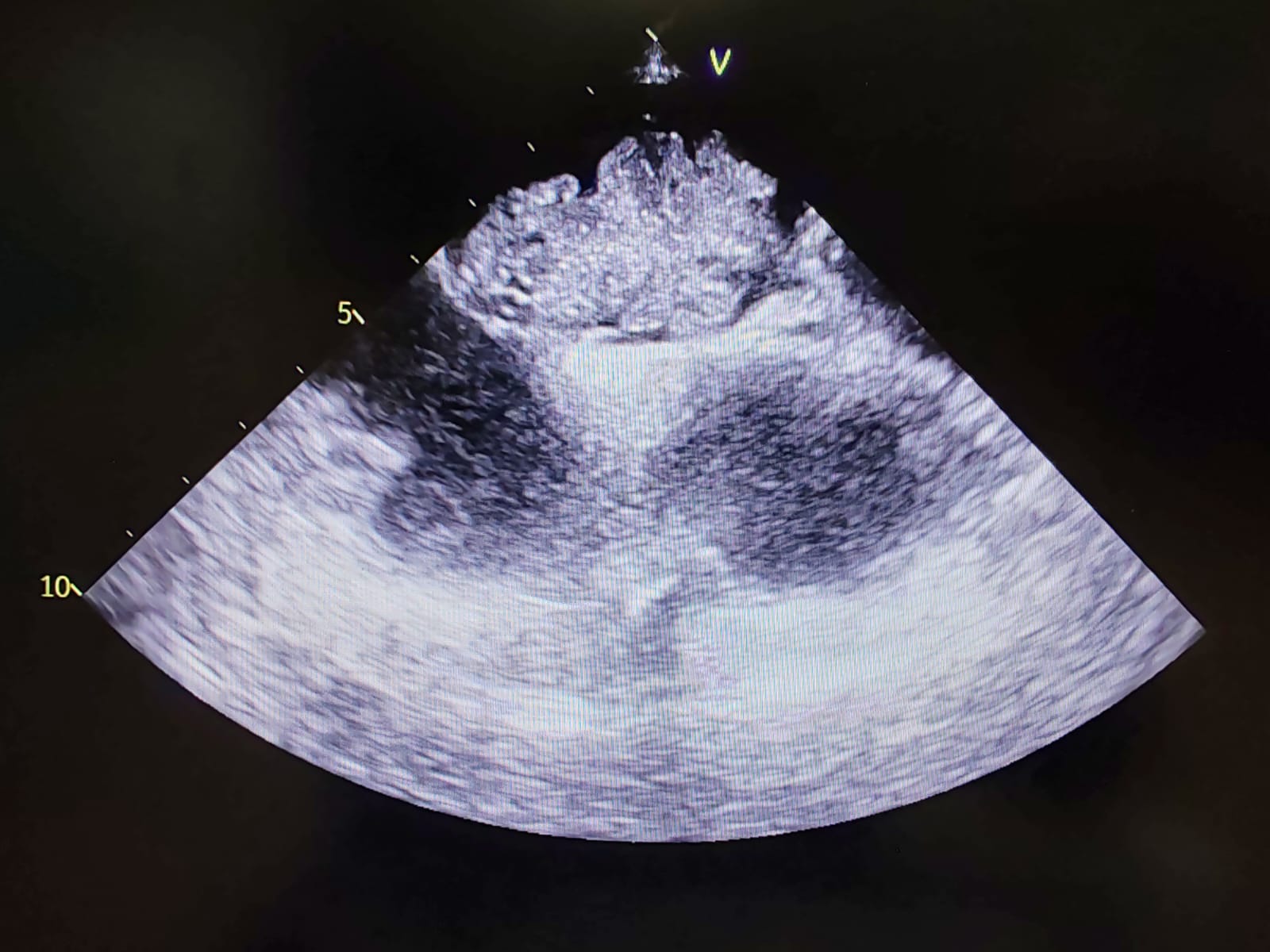
Atrial myxomas are the most common benign primary cardiac tumors, with an incidence of approximately 3 in 1000 patients. Most arise in the left atrium and may cause complications such as obstruction or embolization. We report a case of an incidental left atrial myxoma detected in a patient presenting to the emergency department cause of palpitations. Case Presentation A 51-year-old woman presented with palpitations and hypotension. Her history was notable for thrombocytosis of unclear etiology, under diagnostic evaluation. Electrocardiography revealed sinus tachycardia at 130 bpm, frequent premature ventricular beats. Transthoracic echocardiography showed an isoechoic left atrial mass measuring approximately 3 × 2 cm, initially suspected to be a thrombus. She was admitted to the cardiology unit and started on continuous intravenous heparin. Transesophageal echocardiography demonstrated a heterogeneous, multilobulated, mobile mass attached to the left side of the interatrial septum, measuring 3.8 × 1.9 cm, protruding into the left atrium and prolapsing into the left ventricle during diastole, with high embolic potential. Due to hemodynamic instability and the risk of embolization, she was urgently transferred for cardiac surgery. Surgical excision led to hemodynamic stabilization, and histology confirmed an atrial myxoma. The postoperative course was uneventful, and she was discharged asymptomatic in good condition. Discussion Atrial myxomas most often arise in the left atrium and present variably, including arrhythmias, hemodynamic compromise, or embolic events. In this case, thrombocytosis initially suggested thrombus formation. Transesophageal echocardiography was critical in identifying the mass’s attachment, mobility, and diastolic prolapse, indicating high embolic risk and supporting the diagnosis of myxoma. These findings prompted urgent surgical intervention. Conclusions This case emphasizes the need to consider atrial myxoma in the differential diagnosis of left atrial masses, even in patients with prothrombotic conditions. Transesophageal echocardiography is essential for accurate diagnosis and risk assessment. Prompt surgical excision prevents complications and ensures favorable outcomes.