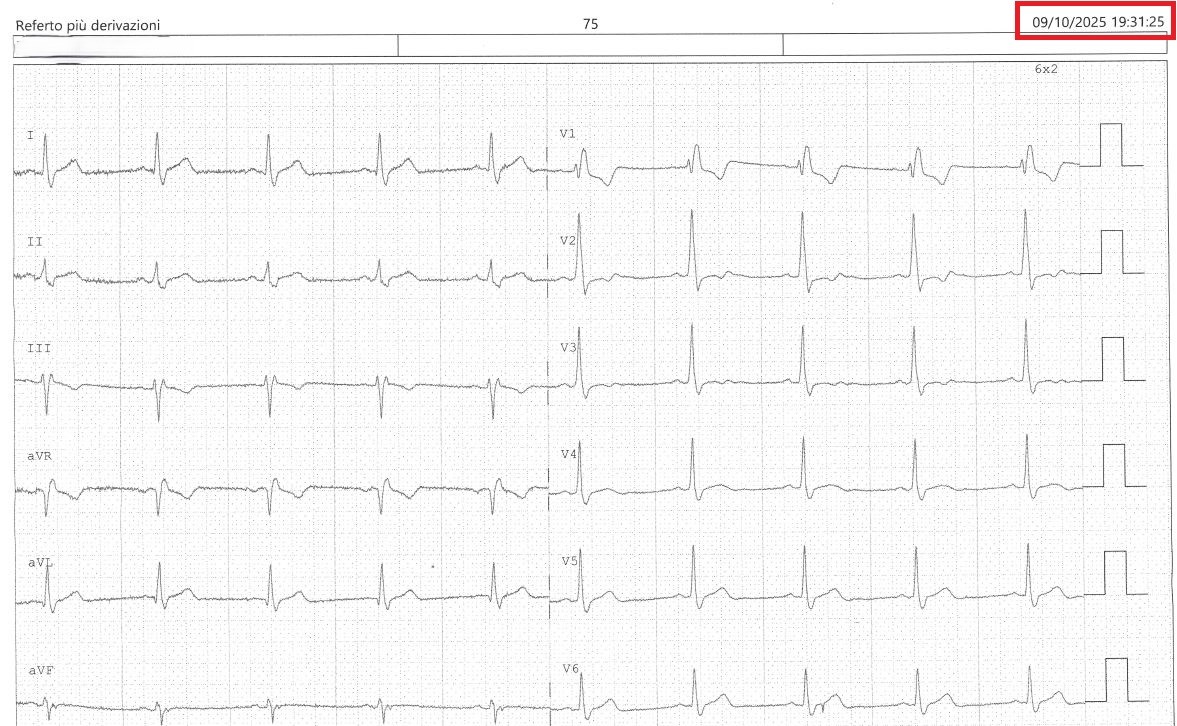
Background Myocardial Infarction with Non-Obstructive Coronary Arteries (MINOCA) is a challenging clinical scenario because of its heterogeneous aetiologies. Among the clinical conditions considered causes of MINOCA, epicardial coronary artery spasm (variant angina, Prinzmetal angina) should be considered, especially when symptoms occur at rest. Abstract Herein, we describe a case of a 51-year-old man who presented to the local emergency department with many episodes of chest pain at rest, followed by rapid palpitations and dizziness. During cardiological evaluation, the patient was asymptomatic, with grade 1 hypertension, without symptoms or signs of heart failure. The echocardiogram was unremarkable, while the electrocardiogram (ECG) demonstrated right bundle branch block with T waves in V1 to V3 initially negative, then positive (Figure 1). Blood tests showed a rise in troponin T from 53 to 205 ng/l, with no alterations in hemoglobin or renal function. Based on these findings, the young man was hospitalized in Coronary Intensive Care Unit. Coronary angiography showed < 50% stenosis of the anterior descending artery and right coronary artery, without any left ventricular wall motion abnormalities or elevations in end-diastolic left ventricular pressure. A diagnosis of MINOCA was established, so the patients underwent cardiac magnetic resonance, but even this investigation was normal. One day, after dinner, the patients alerted the medical staff because of constrictive chest pain, followed by palpitations. Telemetry monitoring showed a 4-minute transient ST elevation, followed by rapid, polymorphic ventricular tachycardia (Figure 2). After ST resolution, the ECG was normal (Figure 3). Therapy with diltiazem and nitrates was established, without further episodes of transient ST elevation. Because of the presence of rapid, polymorphic ventricular tachycardia during epicardial coronary spasm, a bicameral implantable cardiac defibrillator (ICD) was implanted to titrate Ca-antagonist therapy. Conclusions Vasospastic angina is a potentially life-threatening condition that should always be considered in the MINOCA clinical setting. During transient ST elevations, rapid and polymorphic ventricular arrhythmias can occur, so ICD implantation should be considered to protect patients from sudden death.