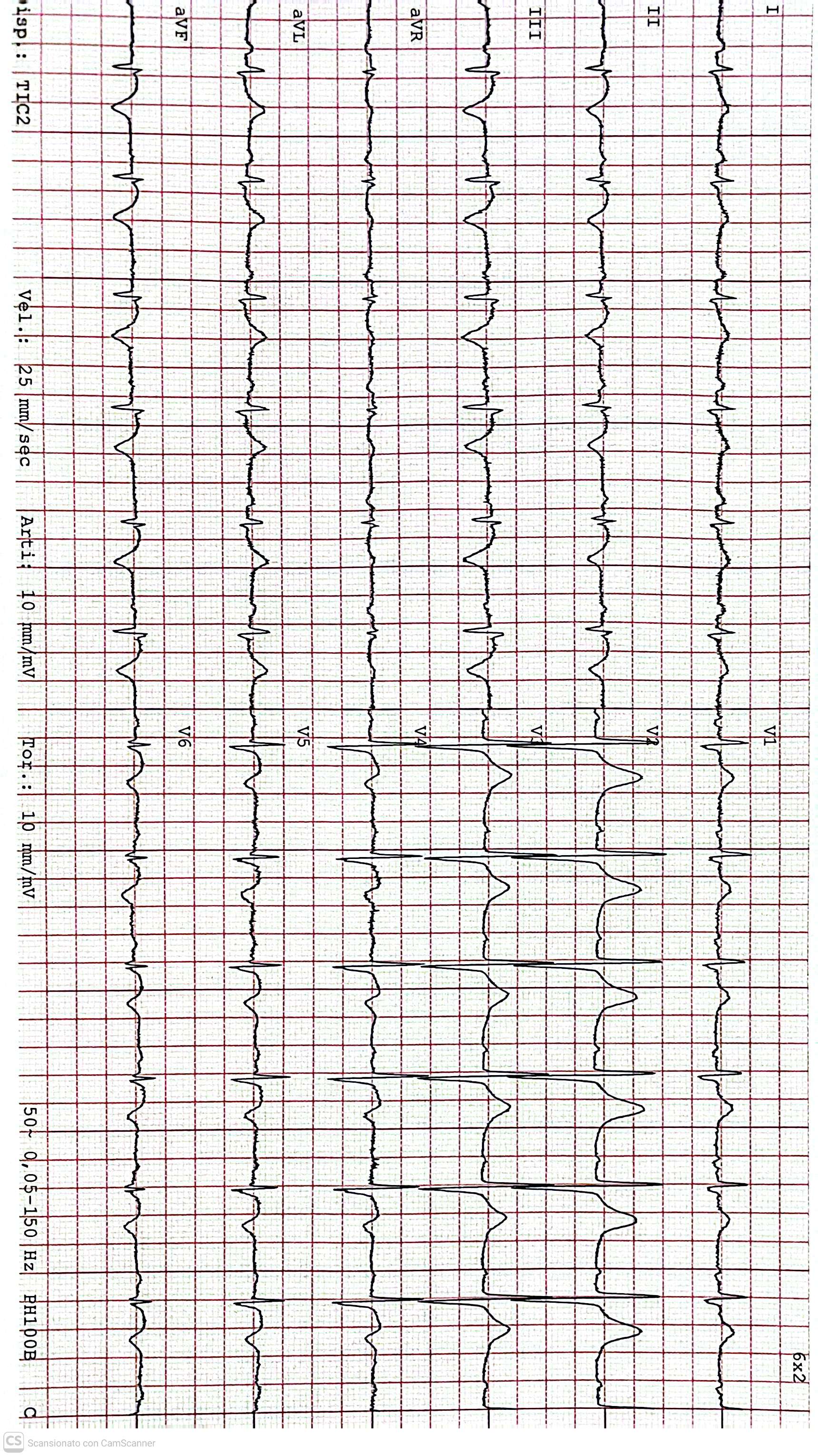
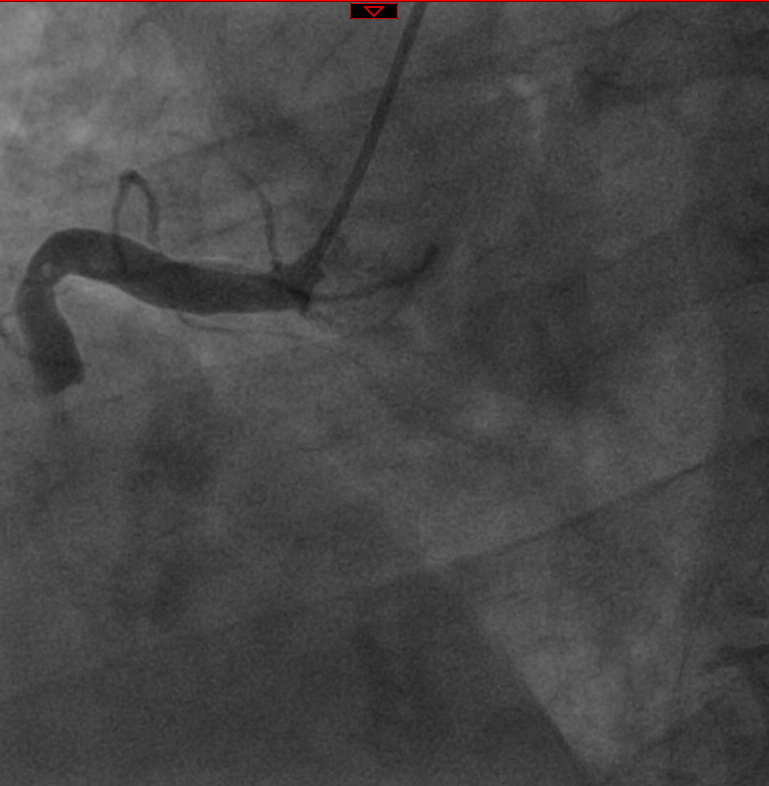
We report the case of a middle-aged man with severe hemophilia A poorly responsive to conventional treatment and multiple cardiovascular risk factors who presented with an infero-lateral ST-segment elevation myocardial infarction (STEMI). (Figure 1). Upon admission, echocardiography showed severely reduced left ventricular function, and an apical thrombus. (Figure 2) Emergency coronary angiography was performed, revealing a thrombotic occlusion of the right coronary artery in the context of aneurysmal vessels, and critical stenoses of the left anterior descending and circumflex arteries. (Figure 3) Several attempts at percutaneous revascularization failed due to unfavorable anatomy and lack of distal reperfusion. Anticoagulation was initiated with strict monitoring, maintaining factor VIII levels above 50% through targeted replacement therapy, and serial imaging showed persistent regional wall-motion abnormalities, but progressive resolution of the ventricular thrombus. Given the coexistence of severe bleeding risk, intracardiac thrombus, and complex coronary anatomy, the case was discussed by a multidisciplinary Heart Team, including hemophilia specialists, and surgical revascularization was preferred over further percutaneous interventions. The patient underwent off-pump minimally invasive direct coronary artery bypass grafting with left internal mammary artery grafting to the left anterior descending artery. The postoperative course was uneventful, with stable factor VIII levels, no major bleeding, and no need for transfusion. Warfarin and aspirin were safely reintroduced and maintained under hematologic supervision. This case highlights the complexity of managing STEMI in patients with severe hemophilia emphasizing the importance of coordinated multidisciplinary decision-making. It also demonstrates that, when carefully planned with adequate coagulation support, minimally invasive surgical revascularization can be safely performed and can be a valid alternative in such high-risk patients.