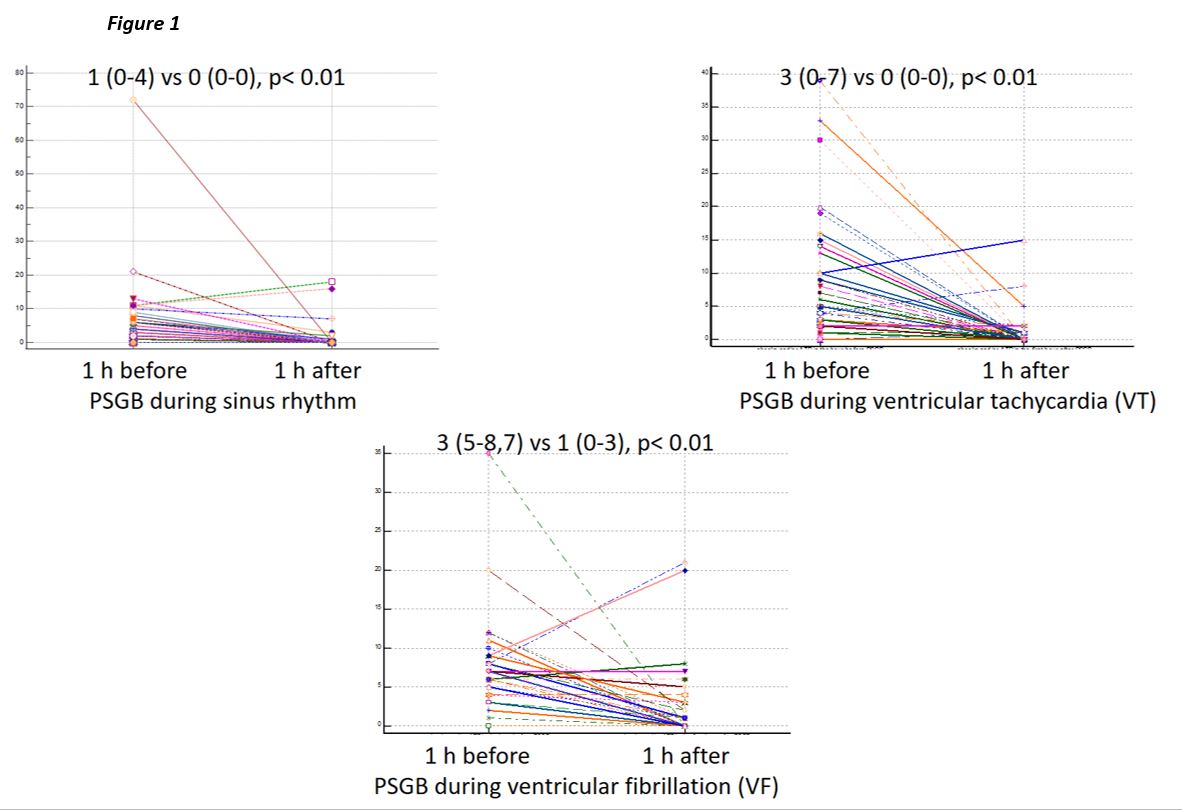
Introduction Percutaneous Stellate Ganglion Block (PSGB) has an increasing role in the treatment of patients with ventricular electrical storm. Multicentre observational studies have confirmed its efficacy and safety, but there is a lack of data on how heart rhythm at the time of the procedure may influence its effectiveness. Materials and methods We considered the PSGBs performed from 01/Jul/2017 to 30/Apr/2024 at the 19 Italian Centres of the STAR consortium. The number of arrhythmias treated with shock (internal or external) or with antitachycardia pacing (ATP) one hour before and one hour after each procedure was compared, both those performed during sinus rhythm and those performed during ventricular arrhythmia. Univariate and multivariate logistic regression models were used to test the association between heart rhythm at the time of PSGB and the probability of complete suppression of arrhythmias in the hour following the procedure. Results During the study period, 180 patients were treated with a total of 254 PSGBs: 100 (40%) during sinus rhythm, 87 (34%) during ventricular tachycardia (VT), 32 (13%) during ventricular fibrillation (VF), 33 (13%) during other rhythm (2 unknown cases). PSGB was shown to significantly reduce the arrhythmias treated both when performed during sinus rhythm and during VT or VF (Figure 1). On univariate analysis, performing PSGB in sinus rhythm was associated with the probability of having complete suppression of treated arrhythmias in the hour following the PSGN [OR 3.8 (1.6-8.9), p<0.01]. However, after correction for both tachycardia cycle and the number of arrhythmias treated in the hour before the PSGB, sinus rhythm at the time of block was no longer associated with the probability of arrhythmia suppression [OR 1.4 (0.5-3.8), p=0.48]. Conclusions This study confirmed that PSGB is effective in reducing the number of treated ventricular arrhythmias both when performed in sinus rhythm and during ventricular arrhythmias. Furthermore, the heart rhythm at the time of block is not independently associated with the probability of arrhythmia suppression in the hour following the procedure. These findings may guide the operator to perform the procedure regardless of the patient's rhythm.