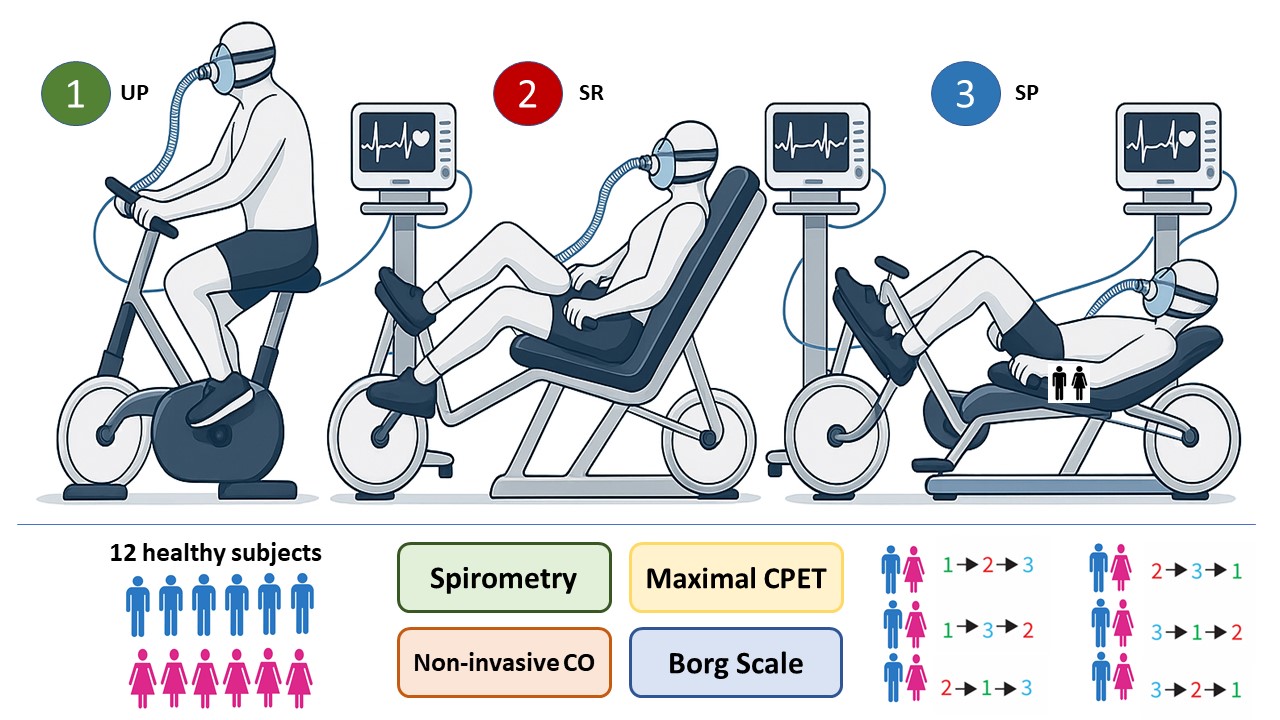
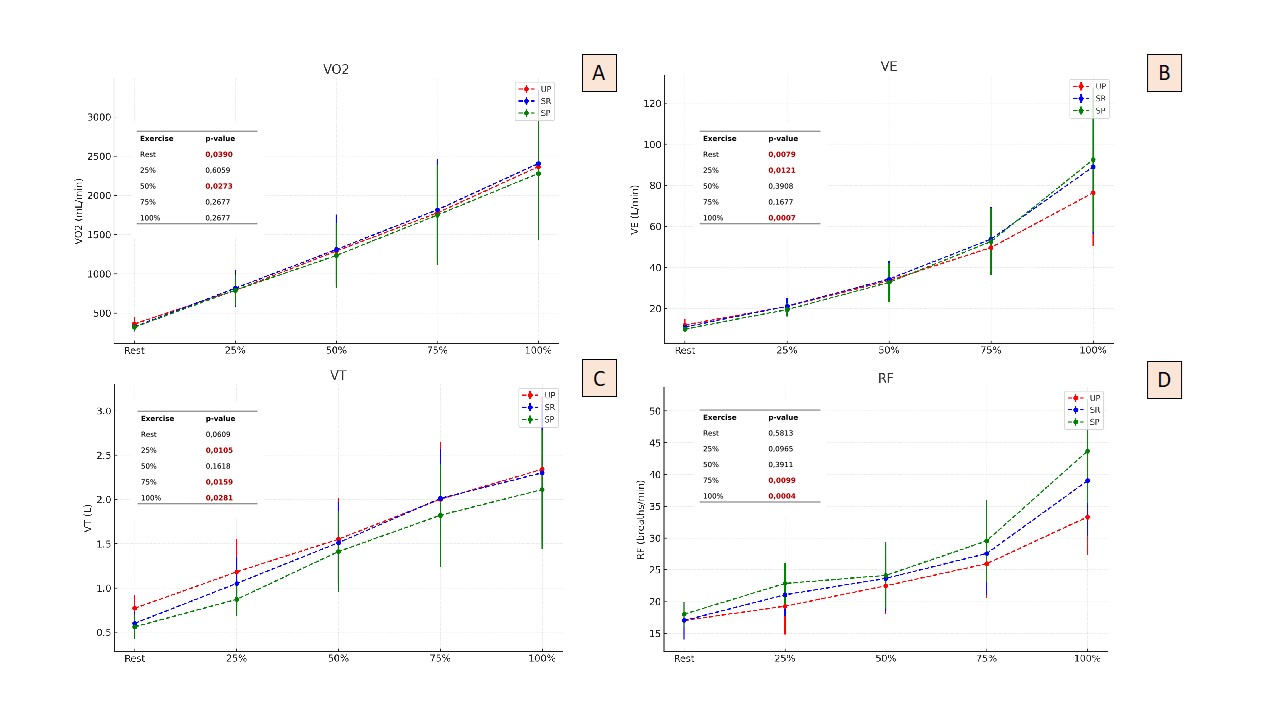
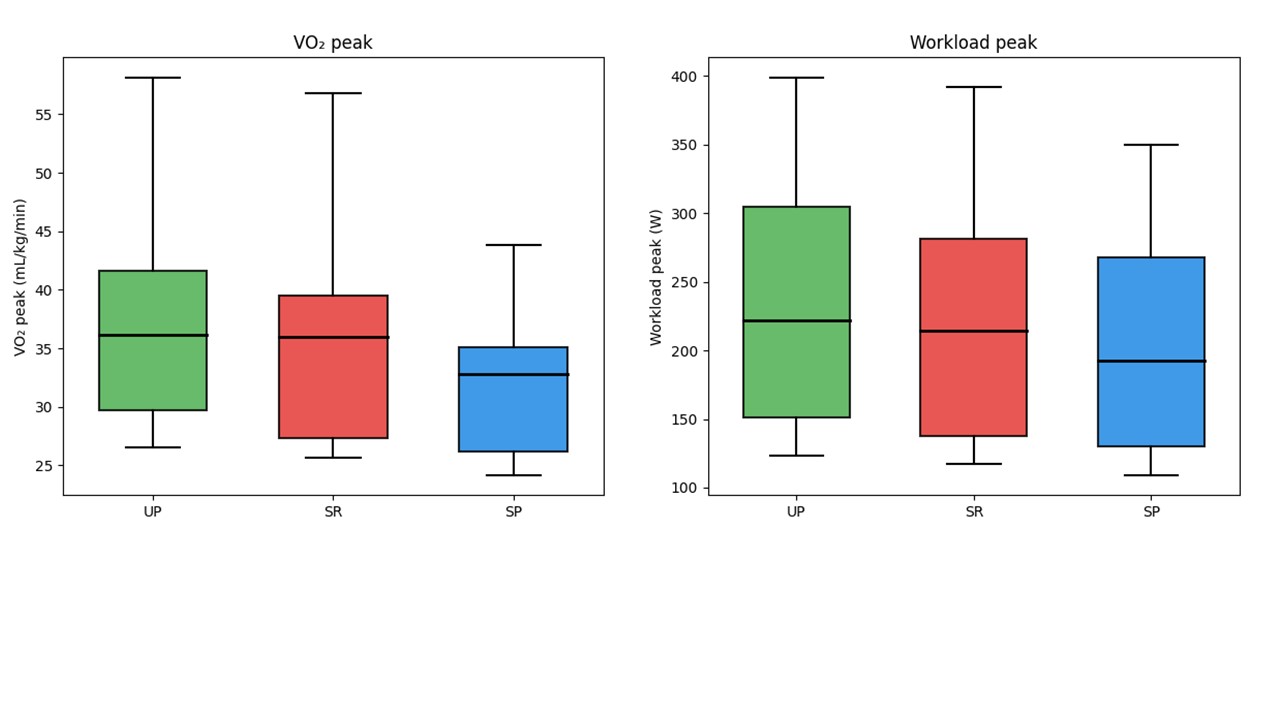
Background : Cardiopulmonary Exercise Testing (CPET) is the gold standard for the integrated assessment of cardiovascular, respiratory, and metabolic function during exercise. Physiological responses may vary according to body posture: upright (UP), supine (SP), and semi-recumbent (SR). Previous studies have reported differences in CPET parameters (VO₂peak, VE/VCO₂ slope, anaerobic threshold, O₂ pulse, peak heart rate), but the available evidence remains heterogeneous and does not allow definitive conclusions. Moreover, non-invasive hemodynamic monitoring through thoracic bioimpedance (PhysioFlow®) enables the assessment of cardiac parameters (stroke volume, cardiac output, cardiac index) during exercise. A standardized comparative analysis of UP, SP, and SR postures, integrating both respiratory and hemodynamic data, is therefore crucial to improve CPET interpretation and to support the development of shared operational protocols. Methods : Twelve healthy subjects (30.9±4.4 y/o, 50% females) were enrolled and randomly assigned to perform three CPETs in different postures: UP, SP, and SR. Throughout all CPET sessions, non-invasive hemodynamic monitoring was performed using PhysioFlow®, and perceived exertion was assessed with the Borg scale. Data were collected and analyzed at baseline, anaerobic threshold, intermediate exercise steps, and peak exercise. Results : At rest, significant reductions were observed in heart rate (HR, p = 0.002; p for trend = 0.007) and a decreasing trend in VO₂ and VE, mainly explained by lower tidal volume (VT) with stable respiratory rate (RR). At the anaerobic threshold, VO₂ values were reduced (p for trend = 0.017) with evidence of an earlier threshold across positions. At peak exercise, VO₂ remained significantly lower, while cardiac output (CO) showed no significant variation despite the decrease in watts. Dyspnea perception, measured by the Borg scale, significantly decreases at peak exercise in parallel with the reduction in workload (watts). Conclusions : SR and SP positions are associated with a progressive reduction in exercise performance, while cardiac output remains stable. The functional limitation appears to be driven by a reduction in tidal volume. Further iso-watt comparisons are underway.