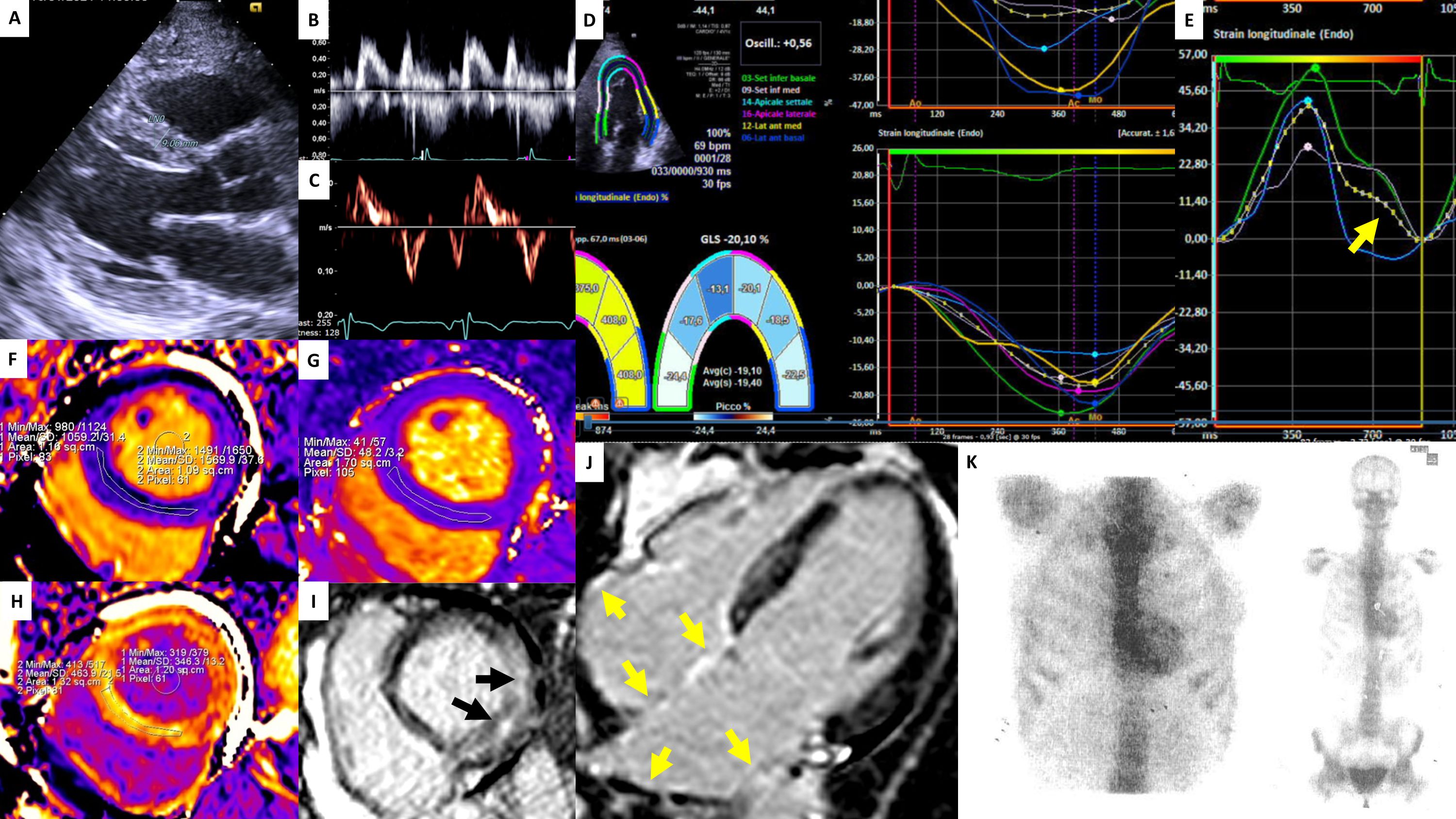
A 48-year-old woman carrying the heterozygous Glu89Gln mutation in the TTR gene, with a family history of hereditary transthyretin amyloidosis (hATTR), underwent cardiac evaluation. She was asymptomatic from a cardiac standpoint, aside from a prior bilateral carpal tunnel syndrome, a common early manifestation of ATTR amyloidosis. Cardiac biomarkers (troponin and NT-proBNP) and the ECG were within normal limits. Transthoracic echocardiography showed normal ventricular size and wall thickness, preserved diastolic function, a GLS of –20%, and normal atrial strain, with no evidence of infiltrative cardiomyopathy. Given her genetic background, cardiac magnetic resonance imaging was performed, revealing a mildly elevated native T1 (1059 ms), normal T2 values, and an increased extracellular volume (ECV) of 32%, consistent with early interstitial expansion. Late gadolinium enhancement demonstrated a non-ischemic pattern, most pronounced in the basal lateral wall, along with biatrial enhancement, findings suggestive of subclinical amyloid infiltration. 99mTc-DPD scintigraphy showed Perugini grade 2 myocardial uptake, which—together with a pathogenic TTR mutation—allowed a non-biopsy diagnosis of ATTR cardiac amyloidosis according to the Gillmore algorithm. The patient was subsequently started on Tafamidis. This case highlights the pivotal role of multimodality imaging in TTR mutation carriers: while echocardiography, strain analysis, and biomarkers may remain normal in the earliest stages, CMR tissue mapping and bone-tracer scintigraphy enable the detection of subtle amyloid infiltration, supporting timely initiation of disease-modifying therapy.