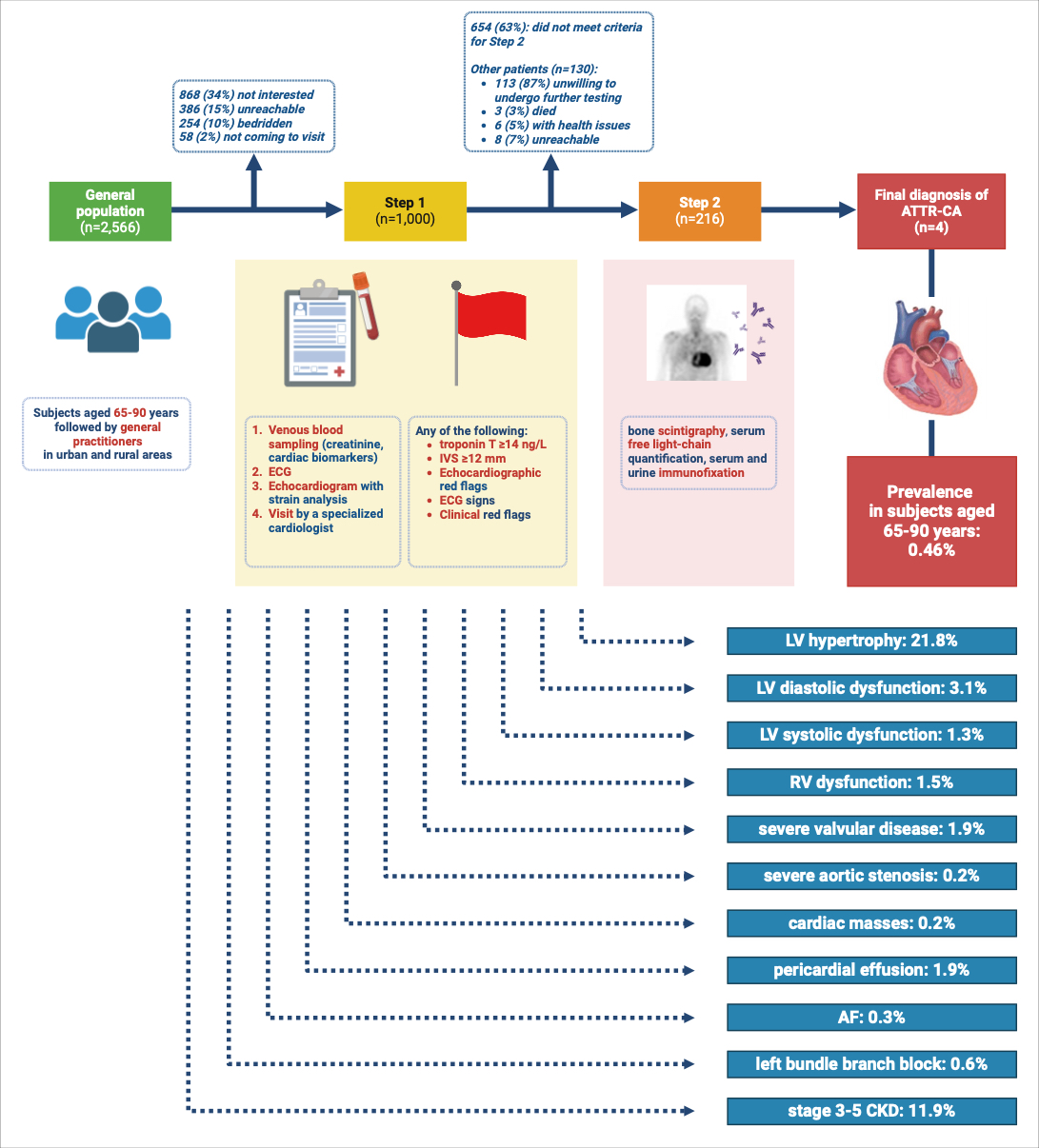
Background The CATCH study investigated for the first time the prevalence of cardiac amyloidosis (CA) in an unselected elderly population. General practitioners proposed screening for wild-type transthyretin cardiac amyloidosis (ATTRwt-CA) to all their patients aged 65–90. We sought the following red flags: interventricular septal thickness ≥12 mm, echocardiographic, electrocardiographic (ECG), clinical signs of CA, or troponin T ≥14 ng/L. Among the 346 subjects with red flags, 216 were tested for monoclonal proteins and bone scintigraphy. 0.46% of patients were diagnosed with ATTRwt-CA. Besides its primary aim, the study provided insights into undiagnosed conditions. Methods We investigated the prevalence of newly detected diastolic and systolic dysfunction, valvular heart disease, other abnormal echocardiographic findings, arrhythmias, and chronic kidney disease (CKD). Results The CATCH cohort included 1,000 participants (51% males, mean age 74 ± 9 years). A hypertrophic phenotype (21.8%) was a red flag for further examination. Echocardiography showed grade II–III left ventricular (LV) diastolic dysfunction in 3.1%, LV systolic dysfunction in 1.3%, and right ventricular dysfunction in 1.5%. One patient diagnosed with dilated cardiomyopathy required a biventricular defibrillator. Severe valvular heart diseases were detected in 1.9% – aortic stenosis (0.2%), mitral (1.0%) and tricuspid regurgitation (0.7%). Additional findings included aortic abnormalities (1.7%) – bicuspid valve (0.1%), dilated aortic root (0.7%) and ascending aorta (1.2%) – requiring cardiac surgery in one case. Two masses (0.2%) were identified, later judged as benign following magnetic resonance imaging. Pericardial effusion was found in 1.9%. Atrial fibrillation (AF) was identified in 0.3%, leading to anticoagulation and pacemaker implantation in a patient with bradycardic AF. The left bundle branch block was found in 0.6%; no advanced atrioventricular blocks were identified. Second-level examinations for coronary artery disease were performed in 0.7%. Stage 3–5 CKD was found in 11.9% of subjects. Conclusions CATCH is the first systematic screening to detect CA in the elderly, based on clinical examination, ECG, echocardiography, blood tests, that also uncovered previously undiagnosed conditions. These findings highlight the potential diagnostic value of such a screening program, as early diagnosis enables timely interventions that may improve patient outcomes and quality of life.