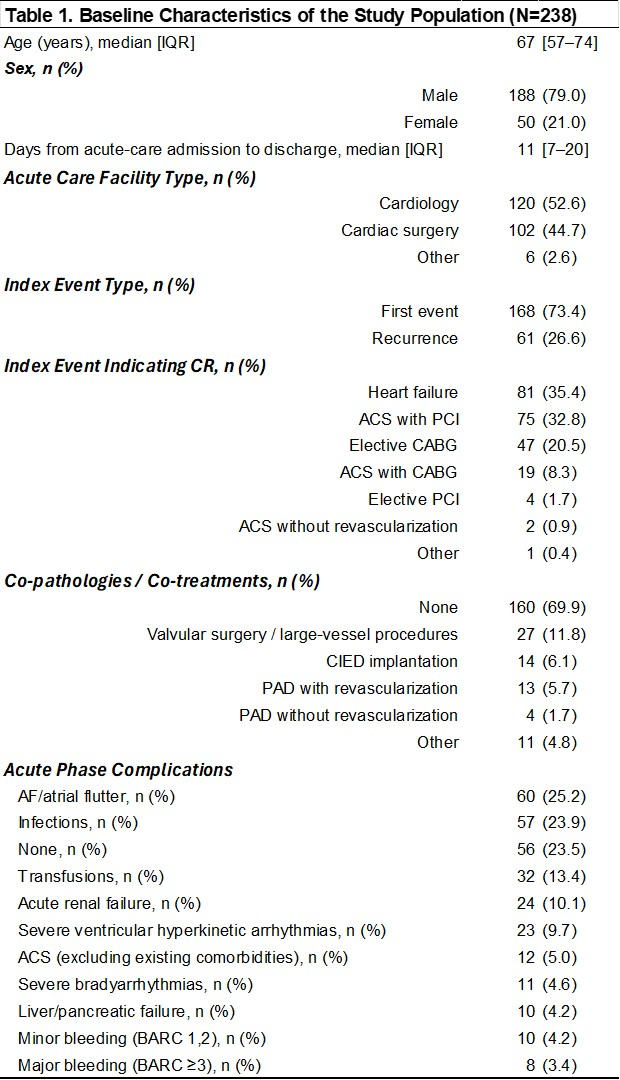
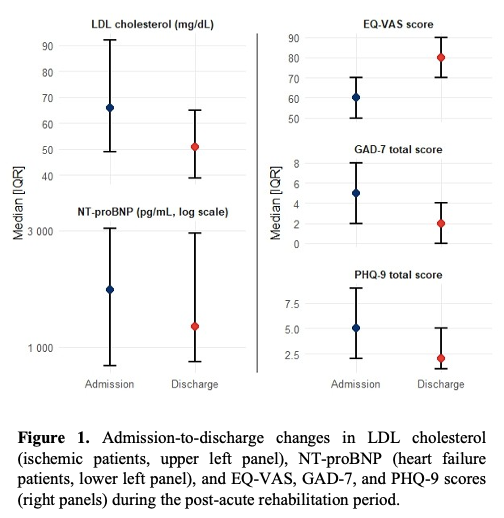
Background, Aims. Cardiac rehabilitation (CR) is the standard of care for patients with coronary artery disease (CAD) and heart failure (HF) in the post-acute phase and represents the most cost-effective secondary prevention strategy. In 2025 the first Italian national prospective multicenter registry on CR in HF and CAD patients was initiated. Aims: 1) to describe CR delivery models for CAD and HF patients in Italy; 2) to evaluate CR effectiveness at program completion and up to 12 months in achieving secondary prevention targets and improving quality of life (QoL). Methods. The registry will collect clinical, biochemical and functional data from 1,600 consecutive CAD and HF patients undergoing CR. Continuous variables are reported as medians (IQR) and categorical variables as counts and percentages. The primary outcome is change from admission to discharge in NT-proBNP (HF) and LDL cholesterol (LDLc, CAD). Secondary outcomes include therapeutic adherence, functional capacity, QoL, psychological status, mortality, hospitalizations and major adverse cardiovascular events. Results. To date, 238 patients were enrolled in 9 of 23 centers (35.4% HF, 64.6% CAD) with discharge data available for 184 patients. Given the preliminary and incomplete dataset, analyses are descriptive. At admission BNP was 233 pg/ml (IQR 130–442), NT-proBNP 1721 pg/ml (IQR 836–3064); discharge values, where available, showed a lower trend (NT-proBNP 1215 pg/ml [IQR 868–2926]). LDLc decreased from 66 mg/dl (IQR 49–92) to 51 mg/dl (IQR 39–65). At baseline, quality of life was assessed with HeartQoL and KCCQ, with scores of 26 and 58, respectively, alongside perceived health status measured by EQ-VAS (score 60). Anxiety and depression scores measured by GAD-7 and PHQ-9 were both 5; cognition MoCA was 26. At discharge, GAD-7 and PHQ-9 scores changed to 2, EQ-VAS to 80, MoCA score was 25. Functional autonomy and frailty also changed (Barthel Index from 90 to 100 and RCS-E from 11 to 1). Conclusions. These preliminary real-world data describe the multidimensional profile of patients undergoing CR in Italy and suggest favourable trends from admission to discharge across biochemical, functional, psychological and QoL domains. A nationwide CR registry may optimize the cost-effectiveness of cardiovascular care by improving target control, therapeutic adherence, functional recovery and QoL, potentially improving number and duration of rehospitalizations and efficient resource utilization.