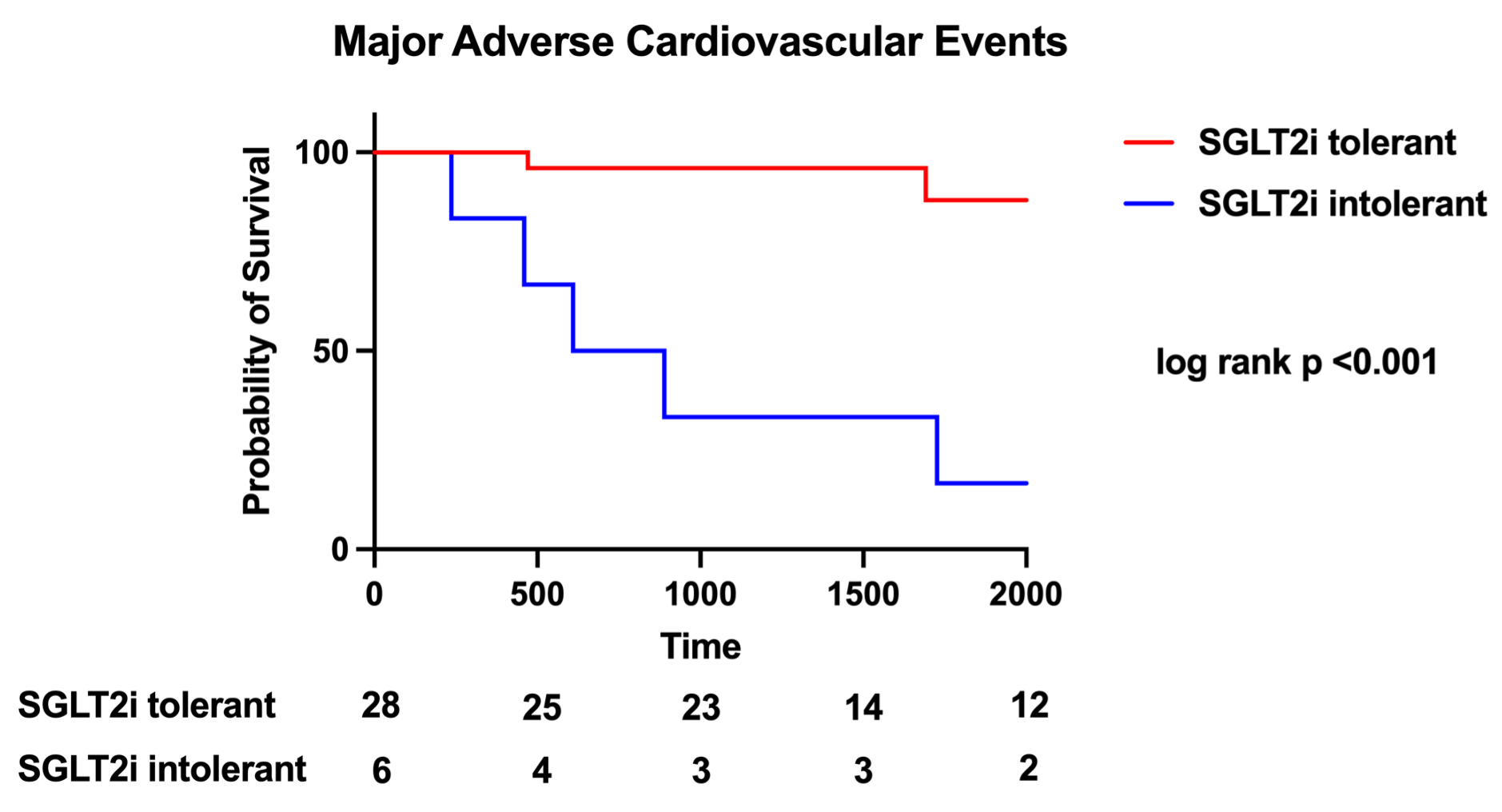
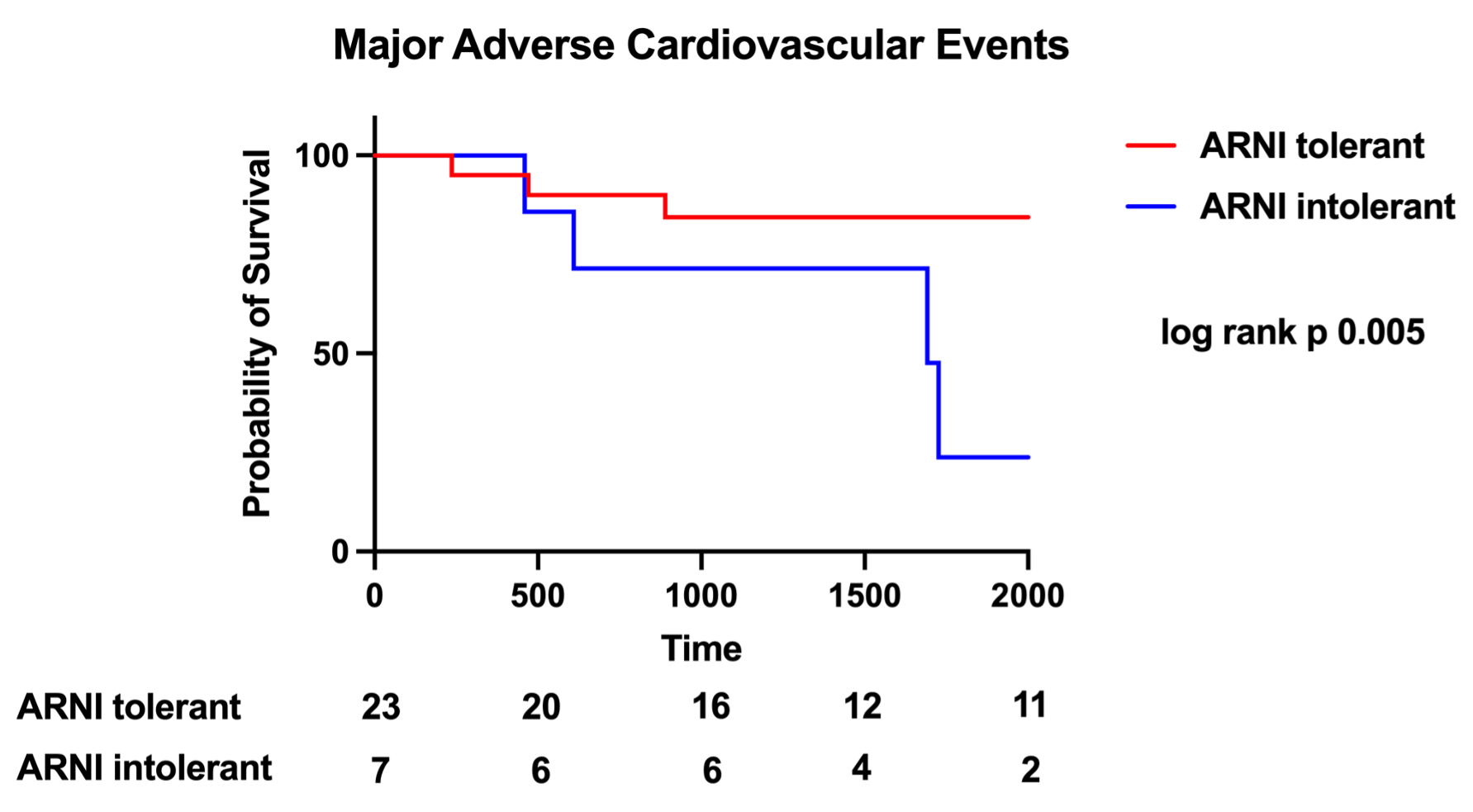
Background : Cardiomyopathy is a leading cause of morbidity and mortality in Duchenne muscular dystrophy (DMD), yet evidence guiding the use of contemporary heart failure (HF) therapies—particularly angiotensin receptor–neprilysin inhibitors (ARNI) and SGLT2 inhibitors (SGLT2i)—remains scarce, as DMD patients are systematically excluded from randomized trials. Objectives : To assess the tolerability of ARNI and SGLT2i in adults with DMD-related cardiomyopathy (DMD-CM) and to explore associations between treatment tolerance, cardiac remodelling, and major adverse cardiovascular events (MACE). Methods : We retrospectively analysed adult DMD patients enrolled in the Molinette-HF ambi-spective registry. Patients were stratified based on tolerance to ARNI and SGLT2i. The primary endpoint was MACE (all-cause mortality, HF hospitalization, arrhythmic storm, ischemic stroke/TIA). Secondary endpoints included individual MACE components and 1-year echocardiographic changes. Results : Among 40 male patients (mean age 22.9 ± 10.1 years), 28 tolerated SGLT2i and 23 tolerated ARNI. Intolerance to either therapy was strongly associated with a more advanced cardiac phenotype at baseline, including markedly reduced LVEF, larger LV volumes, more significant mitral/tricuspid regurgitation, and impaired RV function. During follow-up, MACE occurred in 83.3% of SGLT2i-intolerant vs. 10.7% of tolerant patients (p < 0.001) and in 71.4% of ARNI-intolerant vs. 12.9% of tolerant patients (p = 0.01). Mortality was significantly higher in intolerance groups for both therapies. Echocardiography at 1 year showed stability of LV volumes and diastolic parameters in tolerant patients, whereas intolerance was associated with progressive ventricular dilatation and worsening filling pressures. Conclusions : In this real-world DMD-CM cohort, ARNI and SGLT2i were generally well tolerated and their tolerability identified patients with markedly improved clinical trajectories, lower mortality, and attenuated cardiac remodelling. Conversely, intolerance was a surrogate of advanced myocardial disease and predicted poor outcomes. These findings support the feasibility and potential benefit of incorporating ARNI and SGLT2i into DMD-CM management and highlight the urgent need for dedicated multicentre randomized trials in this underserved population.