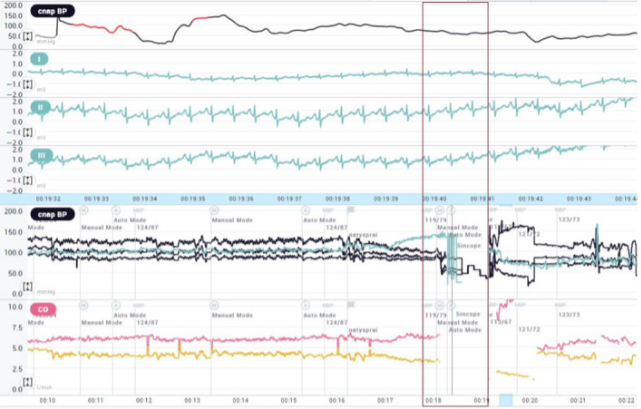
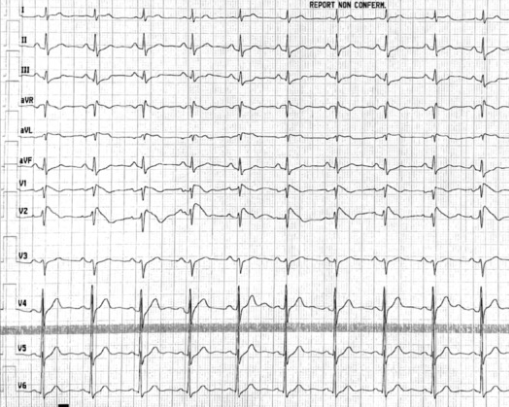
Case presentation: A 53‐year‐old man, with no family history of sudden cardiac death (SCD), was admitted to the Emergency Department for transient of loss consciousness (TLOC) and facial trauma. The TLOC occurred at rest, in an upright position, without prodromes and/or specific triggers. At admission, the body temperature was 37.8°C. The ECG showed a pattern compatible with the type 1 Brugada pattern. The patient was referred to Cardiology Unit for arrhythmic risk stratification. After 2 days of hospitalization a transition from type 1 to type 2 Brugada ECG pattern occurred. No electrocardiographic risk markers for ventricular fibrillation (VF) were present. The late potentials on the signal‐averaged electrocardiogram (SAECG) were negative. No arrhythmic events were recorded at the in‐hospital telemetric monitoring. The clinical interpretation of TLOC without prodromes in patients with the type 1 Brugada pattern was not univocal (arrhythmic or not), such as the patients' management (conservative or invasive). Head‐up tilt test (HUTT) performed showed the induction of vasodepressive syncope without prodromes. An endocardial three‐dimensional (3D) map of the right ventricle was constructed and the programmed ventricular stimulation (PVS) at two ventricular sites, with up to three premature extrastimuli was performed. At unipolar and bipolar voltage mapping in sinus rhythm and at the propagation map, no abnormalities were shown. The PVS was negative for the induction of ventricular arrhythmias. Finally, some doubts remained about the etiology of syncope, and a long‐sensing vector loop recorder (ILR) was implanted. The patient was discharged with the diagnosis of vasodepressive syncope in need of physical counterpressure manoeuvres and tilt training. At 12 months follow‐up, there were no arrhythmias at ILR monitoring or syncopal recurrence. The next‐generation sequencing‐based gene panel test for cardiovascular genomics, including the SCN5A gene, was negative for BrS pathogenic variants. Conclusion: the use of an ILR should be considered in patients with Brugada pattern and unexplained syncope; and in BrS patients with low/intermediate risk, it can help guide the management and ascertain the cause of unexplained syncope. A careful comprehensive evaluation aiming to exclude the correlation between arrhythmic events and clinical symptoms should be considered in the patients' centered care of subjects with type 1‐induced BrS pattern.