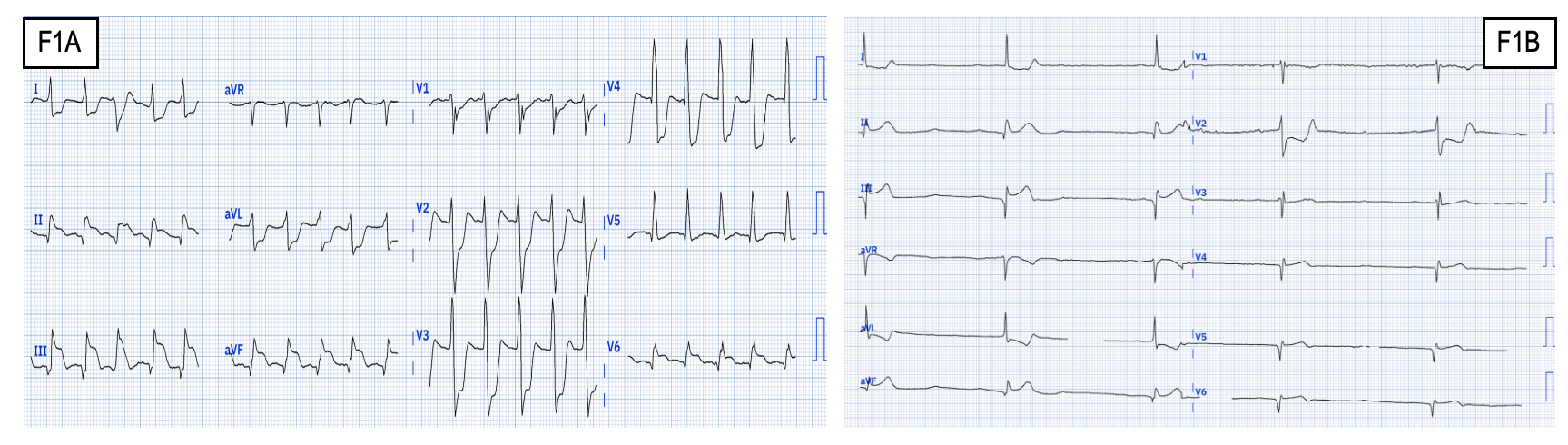
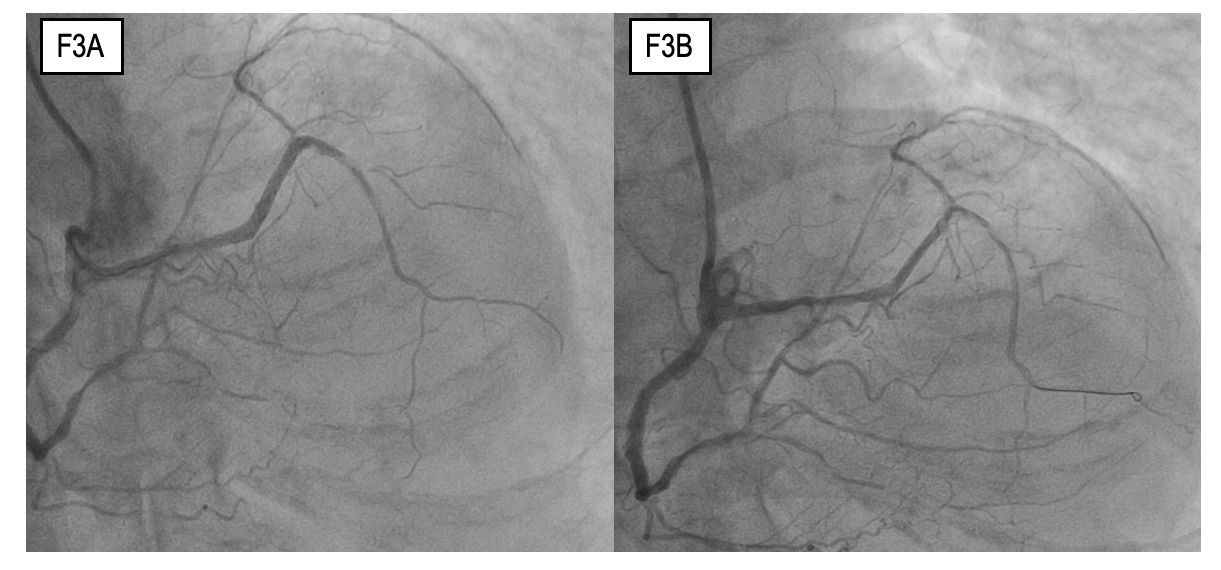
A 76-year-old man presented to the Emergency Department with chest pain. Initial ECG revealed an inferior-posterior STEMI complicated by complete atrioventricular block (F1), leading to cardiogenic shock requiring ionotropic support and temporary pacemaker implantation. Echo showed LVEF 40% and akinesia of the mid-basal inferior and posterior walls. Additionally, an apical 4C view revealed the retroaortic anomalous coronary sign. Coronary angiography demonstrated a rare anatomical finding: a common origin of the left coronary artery from the right coronary artery, constituting a single coronary artery (F2A). Furthermore there were thrombotic occlusion of the mid-distal right coronary artery, successfully treated with two drug-eluting stents (F2B), and significant stenosis of the proximal left anterior descending artery (LAD) (F3A). After hemodynamic stabilization, temporary PMK was removed and a staged PCI of the left main-LAD axis was performed. The procedure was complicated by stent loss, so was used a “deploy and crush” strategy followed by implantation of three drug-eluting stents. However, was occurred a non-flow-limiting dissection on the mid LAD (F3B). The patient’s clinical course was further complicated by multi-organ failure (MOF) requiring continuous renal replacement therapy (CRRT), followed by septic shock, ultimately leading to his death. Anomalous origin of the left coronary artery from the opposite sinus (L-ACAOS), forming a single coronary artery, is a very rare entity with a prevalence of 0.02%-0.15%. The anomalous course of the coronary artery increases the risk of ischemia. Consequently, this anomaly are often associated with poor outcomes, especially in cases of myocardial infarction. Moreover, performing PCI is challenging and carries an increased risk of periprocedural complications. Three reflexions can be made. Timely recognition is critical to achieving a good clinical outcome. Mechanical circulatory support may have benefits, because these procedures can be considered at high risk. Coronary-CT may be a diagnostic tool to differentiate between a benign and a malignant course and to improve revascularization of the non-culprit lesions. This case highlight as anomalous coronary artery from the opposite sinus can complicate the diagnosis and treatment of STEMI with worst outcomes. Few case are present in literature and in all of them there were procedural complications, including ostial dissection and/or cardiogenic shock.